
Warning others after an accident that they could have one too
| Name: | James |
| Field: | Public relations consultant |
| Date: | December 12, 2009 |
| Location: | Washington, U.S. |
comment:
I had a quick question on crisis communication. I’m hoping you can point me in the right direction.
One of our clients is a leading manufacturer and recently had an accident (explosion of secondary tank) at their production facility. Details are still emerging on the cause, but there is a potential that the accident could have been caused by a chemical reaction that is commonly used in the entire industry. As we move forward on communications strategies with them, we are evaluating if the company should take a stance and inform the entire industry of this risk, at the risk of drawing attention to a potentially fatal flaw in a commonly used system – obviously with positive and negative potential impacts to such a stance.
We are in the process of our due diligence/background research on such an approach (has it worked in the past, who else has done it, what are the pros/cons). Do you know of any other examples in which one industry player has made such an announcement that could have impacts on the entire industry?
Peter responds:
In my terms, your problem isn’t so much crisis communication. Your client had a crisis, a high-hazard, high-outrage situation. Now you’re trying to decide whether to do precaution advocacy – to warn others who may face the same high hazard but aren’t experiencing any outrage (concern) yet. And I surmise that you’re worried about whether doing so might arouse some outrage (anger) against your client for blowing the whistle. So it’s a hybrid.
I believe it is established best practice that when a company has an accident, and learns that the cause may be a problem that’s generic and could affect others in the industry, it should notify them in order to prevent additional accidents. A few examples at random:
- In the airline industry it is obligatory to do this sort of root cause analysis and make the results known to other airlines. Regulators routinely put their muscle behind this requirement. After X company has an accident (or even a false alarm) that reveals a specific generic problem, all other companies using the same aircraft are told about the problem and either required or urged to take appropriate action.
- In Canada, Maple Leaf Foods had a food poisoning outbreak in August 2008 that was traced to Listeria contamination in a food slicer. The slicer was constructed in a way that made a particular part hard to clean … and that part ended up harboring the Listeria. The company notified the manufacturer and other companies using the same slicer, and changes were made in the cleaning protocol for that piece of equipment. (Maple Leaf’s handling of its Listeria outbreak has been universally praised.)
- A client in Alaska sandblasted a huge industrial tank, and later picked up high measurements for asbestos inside the tank. It turns out the sandblasting medium (the sand, essentially) contained asbestos. The company immediately notified the manufacturer. When I lost contact with the case, it was considering whether it had a further obligation to notify product safety regulators and the public so that other users of that brand of sandblasting medium would be aware of the problem. I don’t know what it decided, but I know what I think it should have decided.
I’m not an attorney and don’t know the conditions under which a company would have a legal “duty to warn.” But as a risk communication professional, I am confident that the public would hold a company morally culpable if it withheld information about a potentially serious problem, and as a result people in other locations were hurt by the same problem. I think your client is likelier to incur outrage by not issuing such a warning than by issuing it.
Of course it’s important not to go beyond what you actually know. “Preliminary evidence suggests….” “Although we are not yet certain, we decided it was important to let people know what we have learned so far, in order to prevent possible future accidents elsewhere….” If a company reports the results of its investigation accurately, and acknowledges the possibility that further research may lead to different conclusions, it ought to be legally and reputationally safe from claims that it is defaming the manufacturer, damaging public confidence in the operations of competitors, or whatever.
The decision about how broadly to announce what you know (or think you know) may be a difficult one. Do you tell just the manufacturer? The manufacturer and other companies in the industry? Those plus the relevant regulator? Plus the unions representing potentially endangered employees? What about other companies’ shareholders and the general public?
In making these choices, your client should bear in mind that saying too little is a graver reputational risk than saying too much.
One other issue: It’s important that this information be framed in a way that sounds like the company is trying to warn others about a possible future accident, not trying to escape responsibility for its own past accident. The biggest reputational downside to releasing the information is the possibility of getting accused of trying to wriggle out from responsibility by suggesting that “everyone does it” and “we didn’t do anything wrong that led to our accident.”
You may be interested in the following two-part article from Industrial Safety and Hygiene News:
-
Talking about “What Happened”: Post-Event Risk Communication (Part 1)

- Talking about “What Happened”: Post-Event Risk Communication (Part 2)
Published in ISHN (Industrial Safety and Hygiene News), May 2005, pp. 19–20, and June 2005, pp. 36, 38
The first recommendation in Part 1 is “Tell everyone who should know.” That’s it in a nutshell.
What should we tell people about vaccination if the pandemic wave is ebbing?
| name: | K.M. | |
| Field: | State health policy and planning professional | |
| Date: | November 20, 2009 | |
| Location: | U.S. [state suppressed on request] |
comment:
People in my state health department are asking me what they should say in response to this question: Why get vaccinated when the pandemic H1N1 wave has passed?
Here's the response I drafted for them:
Be Transparent.
- It must be remembered that we are presently in our second wave of disease. The first wave occurred beginning in late April. We were one of the first states to report a confirmed case of H1N1. We are still subject to third and fourth waves of the virus. The more people that get vaccinated, the less chance that these waves will have as severe an impact.
- Summarize the actual impact so far and compare it to a regular flu season to illustrate that it is bad. The perception of people about how mild it is has been is counterproductive.… This will support the first point above.
- A lot of people are concerned about the vaccine for H1N1. So far…. (GIVE adverse event summary to this point in time.) H1N1 is as safe as seasonal vaccines and in fact is essentially manufactured in the same way they are. There is no need to fear this vaccine. This has been specifically noted as one of the reasons people were not going to get vaccinated. Address it up front.
- Get more people like _____ to get vaccinated. Perhaps have an event with highly respected and TRUSTED people who get vaccinated once priority populations are out of the fore. Let people see that others they know and trust are getting it. This will support the previous point also.
- Remind people that they also still need to get the seasonal vaccine. We have yet to move into the peak normal seasonal flu season. Get them both….
Any feedback would be appreciated.
Peter responds:
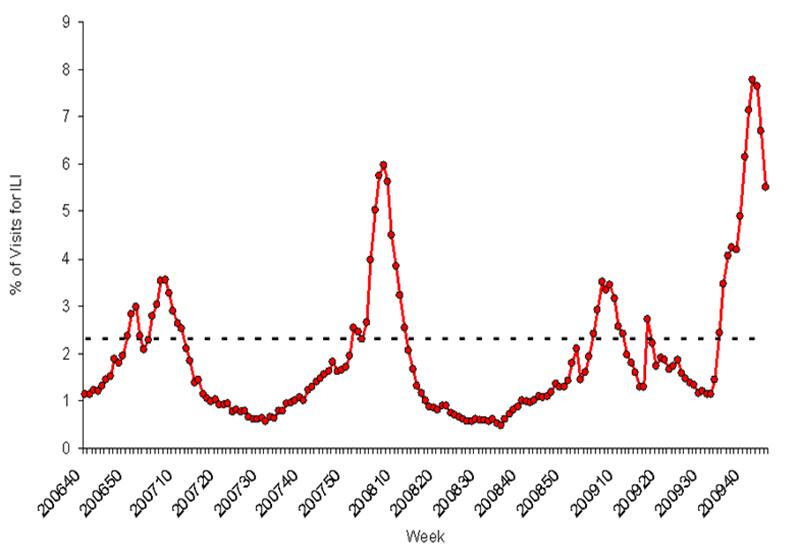
I admire your willingness to be transparent regarding the evidence that the second pandemic wave may be ebbing. As you know, that evidence (on a national level) isn’t unequivocal yet. CDC Director Tom Frieden testified before Congress on November 4 that he thought the wave was peaking and would probably ebb before we had enough vaccine, but then decided the patterns were too varied from state to state to justify such a prediction (yet) and backed off of it. The CDC’s weekly graph of the percentage of doctor visits that were for influenza-like illnesses is still very high, though it has declined significantly over the past three weeks.
So there are really two questions: What do you say now about the possibility that the pandemic wave is about to ebb? And what will you say in a few weeks if it becomes clear that the wave is in fact ebbing?
I agree with you that transparency will be the right response when the evidence is clear. I also think it would be best to warn people now that this may be occurring, rather than appearing to pivot on a dime a few weeks from now from “it’s awful” to “it’s almost over.”
Regarding your proposed answer, I agree that it’s important to ground that answer in uncertainty. Even when we become sure that the second wave is ebbing, we still won’t have a clue whether a third wave is coming. Nor will we know when it will come (if it comes) or what it will look like. It wouldn’t be shocking to see a third wave just weeks after the second … or not till spring … or not till next winter. It wouldn’t be shocking if the third wave came quickly, with little if any warning … or it could creep up on us slowly. Above all, we have no basis for predicting whether the third wave might be more virulent (perhaps even much more virulent) than the second; there’s no evidence of increasing virulence so far, but other pandemics (especially 1918) had later waves that were much more virulent than what had come before, so it’s certainly a possibility.
In the face of all that uncertainty, vaccination (when there’s ample vaccine) makes good sense.
Another important point to make that you didn’t make: People wrongly imagine that the crest of a wave is the end of that wave. In reality, it’s only halfway to the end. When a pandemic wave crests, roughly half the infections, hospitalizations, and deaths attributable to that wave are still to come. There will be plenty of people still getting sick as the second wave ebbs. Unless it ebbs very quickly indeed, some of those people could be protected by post-crest vaccination.
There are two things I don’t like about your proposed answer.

I don’t like your bald claim that the pandemic is “bad” compared to the seasonal flu – and that it is not “mild.” This is compatible with what the CDC is saying, but it is not compatible with the CDC’s own data. Based on the CDC’s November 12 estimates of the number of cases and number of deaths through October 17, the pandemic’s case fatality rate so far is six times lower than the seasonal flu case fatality rate:
- Pandemic: 3,900 deaths divided by 22 million cases = CFR of 0.018%
- Seasonal flu: 36,000 deaths divided by 31 million cases (10% of 308 million population) = CFR of 0.12%
If you look at the CFR separately for people 65 and over versus people under 65, the pandemic’s CFR is a little higher than the seasonal flu CFR for people under 65, and a lot lower than the seasonal flu CFR for people 65 and over. Think in terms of four separate diseases: (1) pandemic flu for under-65s; (2) seasonal flu for under-65s; (3) pandemic flu for 65-and-overs; (4) seasonal flu for 65-and-overs. Then #4 is a killer. By contrast, #s 1, 2, and 3 are all pretty mild – though #2 is a bit milder than #s 1 and 3. That’s the picture the CDC’s data paint. It’s very different from the word picture the CDC is painting, and you propose to paint.

I also don’t like your bald claim that people “still need to get the seasonal vaccine” because we “have yet to move into the peak normal seasonal flu season.” This, too, replicates CDC messaging, but in my judgment it doesn’t live up to your goal of transparency. In past pandemics, the pandemic strain has usually supplanted the previously circulating seasonal strains, becoming the new seasonal strain. The same thing happened in most southern hemisphere countries this time around; Australia and New Zealand, for example, saw very little seasonal flu during their winter season this year. Of course a return of the seasonal strains is likelier if the pandemic ebbs. And even if the pandemic remains, it’s possible that the pandemic and seasonal strains will coexist, at least this season.
Basically, nobody has a clue whether to expect a normal flu season or not. That’s a good enough reason to get the seasonal vaccine, especially for seniors. But you’re no more certain that the seasonal strains will return than you are that the pandemic strain will remain. If you’re going to be transparent about the latter, be transparent about the former too. What you say, in short, should be compatible with the possibility that there may be little or no seasonal flu this year.
Are people apathetic about the environment, or is it something else?
| name: | Cordell Jeffries | |
| Field: | Environmental activist | |
| Date: | November 20, 2009 | |
| Location: | Missouri, U.S. |
comment:
I just read “Watch Out!” and loved it. The problem of apathy has hardly disappeared in the two years since you wrote it.
Eco-apathy is a problem that an organization (http://friendiam.com/) is being created to address. While I would love to talk to you about it in more detail, right now I have a simple-but-hard question to ask.
Has any entity ever credibly computed the number of people on the planet who could be considered apathetic with regard to the environment?
With the number of people with Internet access surpassing one billion people in 2009, as well as an estimated 4.1 billion mobile phones currently on the planet, it would be fascinating to know what the range of answers to that question is. Granted, the information hinges completely on what “defines” environmental apathy.
Any light you can shed on this subject would be appreciated.
Peter responds:
As you say, counting people who are apathetic about environmental issues requires a definition of apathy. There is no obvious boundary between “apathetic” and “interested/concerned” – just a dimension along which environmentalists try to move the public.
Of course there have been opinion surveys on environmental concern at least since the 1960s. The number of people reporting themselves as concerned went up quickly in the early years; it has probably plateaued by now (though I haven’t checked), but at a very high level. Nearly everybody in the developed world (even global warming deniers) claims to be environmentally concerned – and means it; and even can cite behaviors like recycling to prove it. Compare environmental concern with, say, concern about world hunger or HIV or racial justice, and I’m pretty sure you’ll see that environmental concern is more than holding its own.
I realize that this breadth and depth of concern hasn’t been sufficient to motivate the sorts of commitments environmentalists are seeking – for example, willingness to abandon our pursuit of permanent economic “progress” or willingness to make sizable short-term material sacrifices in return for a better environmental prognosis. But calling that problem “apathy” may not be useful. Perhaps it is selfishness, or ignorance, or even ideology (materialism is certainly an ideology, deep-seated in modern consciousness). Perhaps only desperation would motivate the sorts of societal and individual changes many environmentalists now think necessary – and arousing desperation (before it’s too late) isn’t the same as piercing apathy.
An increasing piece of the problem, I think, is denial. If environmentalism requires significant sacrifice of things and values we hold dear, then people may be motivated to eschew environmentalism in order to hang on to those things and values (awhile longer, anyway). That would be desperation itself, not the absence of desperation! And desperation leads to denial.
You might want to read a long column I wrote earlier this year on the ways I think environmental activists may be exacerbating climate change denial in their efforts to fight climate change apathy.
Cordell responds:
Rhetorical concern is easy to quantify, and some results might indicate that apathy (of the 100% pure variety) is “holding its own” at a level one could consider low.
But apathy needs to start being measured in terms of actions, which are also quantifiable. That’s where the proverbial rubber meets the road. And quantification of ecologically motivated action is what I am seeking, even in the form of an educated guesstimate.
Would it be fair to consider raw sales data for less- and non-green products as a somewhat accurate indicator of “action-based” apathy?
If you are wondering where I am going with this train of thought, it is to the simple idea that if every consumer in this consumer culture would purchase the greener version of ONE product in their life from now on, the positive impact on the planet would monumental. And that impact would be multifaceted, one step in the right direction on a litany of eco-issues. I am curious to see if there is a resource for such consumption-driven data.
Peter responds:
I’m not sure how monumental the progress would be if every consumer picked one green product to feel good about buying. The key question, it seems to me, is whether you can help people frame that initial purchase as a behavioral commitment – that is, as evidence that they care about the environment and thus as a foot-in-the-door to more (and deeper) actions in the future.
A lot has been written about the conditions under which people do one thing and then feel free from further obligation (“I gave at the office”) versus the conditions under which people interpret their own initial behavior as just the beginning. To leverage your impact, you will want to read this literature.
Why didn’t President Obama get vaccinated against swine flu? Should he have?
| Name: | David |
| Field: | Public health |
| Date: | November 20, 2009 |
| Location: | Tennessee, U.S. |
comment:
Do you think that President Obama’s decision not to get vaccinated against swine flu was influenced by the backlash that arose following the 1976 swine flu debacle?
Peter responds:
I don’t have any inside information about why President Obama decided not to get vaccinated against swine flu.
But I don’t see how the 1976 swine flu controversy would have led to that decision. It’s true that President Gerald Ford publicized his own swine flu shot in 1976, as part of the launch of the government’s mass vaccination campaign. But Ford wasn’t especially criticized for that. He was criticized for launching the campaign at all – because the vaccine turned out to cause Guillain-Barré syndrome in a small percentage of vaccinees, while the pandemic the vaccine was intended to address never materialized.

This time we’ve actually got a pandemic, albeit a fairly mild one. And while the 2009 H1N1 vaccine may turn out to have problems of its own, it’s very, very unlikely to turn out more dangerous than H1N1 itself.
No, I assume President Obama decided not to get vaccinated for the reason he gave: because the CDC had identified a number of high-priority groups to get first dibs on the vaccine, and the President wasn’t in any of the groups. He didn’t want to be accused of line-jumping.
In terms of the national welfare, that decision makes no sense. We all have a stake in President Obama staying healthy. We don’t really want him laid up with the flu for a week. We certainly don’t want him ending up one of the 30% of hospitalized swine flu patients who had no underlying condition to put them on the CDC’s priority list. Presidents get all kinds of medical attention most of us don’t get … and should.
But the government badly overestimated how much vaccine would be available by now, which has led to lots of public outrage about the inadequate vaccine supply, and lots of complaints about why specific people (from Wall Street bankers to Guantanamo detainees) were slated to get some. I can’t dispute that the President would have taken some flack if he had promoted himself to the head of the line. With vaccine demand so obviously outstripping vaccine supply, it would have been hard for him to sell such a decision as setting a good example for other prospective vaccinees.
The question of whether “important people” should be prioritized for scarce medical treatment is one that has bedeviled ethicists for a long time. If we’re going to privilege the President in that way, what about Senators? Mayors? Cancer surgeons? Cops? Sewage treatment plant managers? A lot of people can make a case that the world shouldn’t have to function without them, even for a week. Contingency plans for a severe pandemic often do prioritize key personnel, aiming to keep them healthy so they can keep society’s overstressed infrastructure going. But with a pandemic this mild, the CDC prioritized only people most at risk, plus those who come into close contact with people most at risk (health care workers and other caretakers of the vulnerable).
Of course if the President comes down with swine flu, he will be criticized for having put public relations ahead of the public’s business.
If he had gotten vaccinated, he’d have been criticized – by pretty much the same people – for jumping the line.
And if he had utilized one of my favorite risk communication strategies and shared the dilemma, asking the public whether he ought to get vaccinated or not, he’d have been criticized for indecisiveness. “No wonder he can’t make up his mind about Afghanistan. He can’t even decide whether to get a flu shot!”
So far he hasn’t been criticized much for going unvaccinated. So as long as he stays healthy, I guess he made the right decision … sort of.
Using DDT against malaria in Africa
| Name: | Happynus Pilula |
| Field: | Student |
| Date: | November 20, 2009 |
| Location: | Tanzania |
comment:
I am interested to know the risk associated with the use of DDT in malaria vector control so as to simplify the risk communication process to the society and stakeholders at large.
Peter responds:
You have three problems here:
- Convincing people to take the risk of malaria seriously enough and to take appropriate precautions against that risk.
- Convincing people not to overreact to the risk of DDT – not to object to its appropriate use against malaria.
- Convincing people to take the risk of DDT seriously enough and to take appropriate precautions against that risk too.
For malaria in general, look at the articles indexed under “Precaution Advocacy (High Hazard, Low Outrage).” Those are the articles focusing on how to convince people to take precautions about a serious risk (like malaria) when the problem is that they are too apathetic about the risk.
Something to keep in mind as you think about malaria precaution advocacy: Especially in developing countries, officials often recommend precautions that are not practical for people to take. Telling people to wash their hands, for example, is frustrating advice in places where clean water is in short supply. Impractical advice undermines the credibility of many health promotion efforts, and it arouses frustration and a sense of futility in the people.
For DDT in particular, the risk communication problem is different and more complicated. As I understand it, DDT is genuinely harmful to the environment, and also genuinely useful against malaria. Other ways of dealing with malaria are less effective and/or more expensive, and thus less practical for developing countries with a serious malaria problem.
Bear in mind that the effectiveness of DDT versus other ways of addressing malaria isn’t a communication question, and you can’t assume I’m right about the answer!
But if I am right, here’s the problem: In richer countries with less serious mosquito-borne diseases – e.g. the U.S. – outlawing DDT made sense. In poorer countries with more serious mosquito-borne diseases – e.g. Tanzania? – outlawing DDT may not make sense. But if DDT is outlawed in the developed world, while DDT manufacturers (also in the developed world) are shipping DDT to developing countries, that arouses all sorts of understandable outrage. Activists in the developed world agitate against the “circle of poison.” People in the developed world may feel guilty. People in the developing world will surely feel envious and discriminated against.
In other words, DDT may make good technical sense in Tanzania’s battle against malaria, but it may arouse so much outrage that the Tanzanian government (not to mention international agencies and donor countries) may find it difficult or even impossible to use because of public resentment.
In this case the problem wouldn’t be too little outrage about malaria, but too much outrage about DDT – which becomes a symbol of Tanzania’s poverty and oppression, and of the double standard of various outsiders (pesticide manufacturers, international agencies, donor nations). Unless the outrage about DDT is managed well, it may be hard to manage the hazard from malaria – and people may die needlessly.
For more on how to handle this sort of situation, see the articles indexed under “Outrage Management (Low Hazard, High Outrage).”
Note that managing DDT outrage well does not mean teaching people (falsely) that DDT risks are trivial. It means teaching people (accurately, I am told) that DDT risks are justified in places where malaria risks are greater and where alternative remedies are more expensive, less effective, or impractical for some other reason. This has to be done sadly, not triumphantly. The message isn’t that people are foolish to worry about DDT, but rather that the malaria situation is dire and Tanzania must make painful choices.
You can see why this is a difficult message to convey – and perhaps impossible for a rich donor nation or a multinational pesticide company to convey. And again I want to stress that it is a sound message only if it is technically accurate; that is, only if it really makes sense for Tanzania to deploy DDT against malaria, given the health, environmental, and economic realities your country faces. That’s a question I am not qualified to judge.
The third problem has to do with minimizing the genuine risks of DDT. If the authorities can manage DDT outrage effectively enough to be able to use the chemical, they will also want to do everything they can to show people what precautions they should take (and what precautions the authorities promise to take) to protect themselves, their families, their animals, and their crops from the DDT.
If people are worried about the DDT, discussing with them what precautions they can take and what precautions the authorities will take is a key aspect of good outrage management. If people are not worried about DDT, then convincing them to take appropriate precautions is, once again, precaution advocacy.
The emerald ash borer: a very tough precaution advocacy problem
| name: | Drew Todd | |
| Field: | State urban forestry coordinator | |
| Date: | October 28, 2009 | |
| Email: | drew.todd@dnr.state.oh.us | |
| Location: | Ohio, U.S. |
comment:
The Emerald Ash Borer (EAB), a non-native insect from Asia, was identified in northwest Ohio in 2003. Since that time, it has spread to over 50 of Ohio’s 88 counties, infesting and killing rural and urban native ash trees. For the past several years, Ohio’s Urban Forestry Program has been helping communities prepare for their inevitable infestation.
We’re attempting to provide awareness and options in hopes that communities would take appropriate and timely action. The environmental and social loss of a community’s public ash trees, which may exceed 10% of its street tree population, pales in comparison to the economic burden of having to remove hundreds of ash trees at the same time.
Many communities have taken our mitigation suggestions, and are systematically removing their ash trees prior to infestation. Unfortunately, many more communities have failed to act. Those communities in northwest Ohio that haven’t proactively removed their ash trees are now requesting our immediate help to convince decision-makers to act.
If possible, we’d like to identify those barriers that inhibit municipal administrators in other parts of our state from failing to take appropriate and timely action. What advice or guidance can you offer to help us overcome this anticipated EAB apathy?
Peter responds:
You’re facing as difficult a precaution advocacy problem as I’ve encountered in some time.
Here’s what you’re up against:
- People discount the future. This is a perennial barrier to many precaution advocacy efforts: It’s hard to persuade people to take action against a problem they don’t face yet. Maybe if the emerald ash borer were advancing inexorably on a specific town in visible ways – three miles away last year, two miles away this year – you might be able to arouse some sense of imminence. But “it’ll get here eventually” isn’t much of a call to arms.
- I’m sorry to say this: Most people are likely to find the EAB issue pretty boring when they hear about it. Getting people to take action against a problem they don’t face yet pretty much requires getting them to imagine the problem. It’s tough enough to get people to imagine a really vivid problem, like a flood or a pandemic, before it’s imminent. Arousing outrage is usually the key to precaution advocacy. But your issue doesn’t have a whole lot of outrage potential. Maybe close-up photos of the EAB can inspire a little dread, or at least a little disgust.

- You have no real precaution to advocate. If I understand you right, you’re not trying to persuade communities to solve their EAB problem by taking prompt action to extirpate the emerald ash borer or protect their ash trees. The problem is unsolvable. The ashes are doomed: ashes to ashes. All you want is for communities to cushion the economic blow of having to remove lots of infested ash trees all at once by preempting the insect and removing the ash trees before they’re infested. Lots of research shows that people are more easily motivated to solve a problem than to mitigate one – especially one they don’t face yet. You’re not offering people ways to prevent the ash borer infestation, not even ways to make it less likely or less unpleasant … just ways to make it less expensive.

- People love their trees, even their publicly owned street trees. But I don’t see any way to harness that love on behalf of your goal of getting communities to kill the trees before they have to. If anything, the love cuts the other way. Imagine trying to persuade people to kill their pets now because they’re going to get sick and die in years to come.
Finally, I’m not convinced that your goal makes sense. You don’t seem to be claiming that the infested ash trees will do actual harm – fall down on cars and pedestrians, for example, or infest other species. You’re just saying that communities can better afford to remove the trees piecemeal than all at once.
But assuming a community waits till the infestation arrives, why will that require it to cut down all its ash trees at the same time? Will they really all get infested the same year? Even if they do, can’t the community take its time removing them? Mightn’t some ash trees withstand the attack and never need to be removed at all? If there really are good reasons why it’ll be necessary to remove all the trees in the same year, why won’t that be cheaper than coming back again and again for more trees? And why can’t a community start putting away money for the job now, but wait to implement until the infestation arrives? Maybe the experts will come up with a solution in the meantime. Even if they don’t, why should the community deprive itself of an amenity prematurely?
There may be good answers to these questions. If so, you need to provide the answers. They’re not obvious on their face, and they’re not in the brief comment you sent me. The burden of proof is on you to convince community leaders and community members that preemptive ash removal is sound policy.
One possible answer: “If we replace our doomed ashes now with saplings of some other species, by the time the EAB hits town we could be well on our way to a new, more resilient canopy of trees.” Another possibility (if it’s true – I’m making up facts here): “Other communities have found it really painful to watch their beloved ashes slowly succumb to the EAB. They’re visibly sick for years before they finally die. It’s less painful in the long run to bite the bullet and replace the trees now.” Or perhaps: “If we cut down healthy trees, they can be used for firewood. If we wait till they’re infested, the wood will be quarantined and will have to be disposed of carefully, expensively, and uselessly instead.”
Still, unless the infested trees are going to do actual harm, I’d be inclined to enjoy my ashes while I can.
Building a policy case for preemptive ash removal is your second task. Your first task is finding a way to gin up some emerald ash borer outrage. It won’t be easy.
There’s an alternative you might want to consider: dilemma-sharing. Instead of trying to sell communities on cutting down their ashes now, make it your goal to warn communities that the EAB is on its way and so far appears unstoppable. Lay out the policy alternatives and the pros and cons of each; describe the reasoning of some communities that have decided on preemptive removal and some other communities that have decided to wait till they have no choice. Define success not in terms of what a community decides to do, but in terms of whether it is aware of the problem and makes a thought-through policy decision (with adequate public awareness and public involvement) on how it wants to proceed.
Among the advantages of this approach: You no longer need to try to arouse more outrage than a neutral, factual description of the situation naturally arouses. With luck (and some skill), the paradox of the risk communication seesaw may come into play. If you’re less committed to persuading people to take action now, they may be likelier to decide that that’s the best option. For sure they’ll be likelier to rely on your information to make their own informed choice.
The meme that this pandemic is “like the seasonal flu”
| name: | Anna Meldolesi | |
| Field: | Science journalist | |
| Date: | October 23, 2009 | |
| Location: | Italy |
comment:
I’m a science journalist working in Italy (www.darwinweb.it). I think the national strategy of communication about pandemic H1N1 in my country is downplaying risks and uncertainties. The claim of the Italian TV advert is: “This pandemic influenza A is a normal flu. It can be best handled by following five rules….”
(If you are interested you can see the TV ad at http://www.wikio.it/video/1796856. ![]() The mouse is a 50-year-old puppet unknown among today’s children. According to the Italian government, 257 TV stations in South America are asking for permission to broadcast the Italian ad.)
The mouse is a 50-year-old puppet unknown among today’s children. According to the Italian government, 257 TV stations in South America are asking for permission to broadcast the Italian ad.)
In my opinion the message becomes: Pandemic flu is equal to seasonal flu and is normal.
Epidemiology says it is not true that pandemic flu is the same as seasonal flu. I don’t know what “normal” means from a scientific point of view, but I guess for laypeople it means you have to do nothing special if something is normal.
I wonder why people should improve hygiene standards and (more important) why they should get their vaccine shots if pandemic influenza H1N1 is normal. Consider that in Italy only 19% of people get vaccinated for seasonal flu every year. Coverage is only 30% among health workers.
May I know your opinion?
Peter responds:
My wife and colleague Jody Lanard collaborated on this response.
We agree with you. Pandemic H1N1 Influenza A is not a normal (that is to say, “average seasonal-type”) flu. Some of the reasons:
- Its epidemiology is radically different so far. The seasonal flu attacks all ages, but roughly 90% of seasonal flu deaths (at least in the U.S.) are 65 or older. The pandemic flu, in stark contrast, infects almost no one over 65, and very few over 50. Meanwhile, people under 65 who catch the pandemic flu have a much higher rate of complications and death than people under 65 have when they catch the (average) seasonal flu strains. And this age difference is even more pronounced when you break the under-65s down into narrower age ranges. In other words, the pandemic so far is much safer than the “normal” flu usually is for the elderly, and significantly more dangerous than the “normal” flu usually is for their children and especially their grandchildren.
- Although we don’t yet know the ultimate attack rate of the pandemic flu virus, far more people are susceptible to it (because they lack any degree of prior immunity) than are susceptible to the seasonal flu strains. However mild or severe the pandemic turns out to be, most flu experts think it will end up more pervasive than the “normal” flu.
- Perhaps most important, the “normal” seasonal flu strains rarely if ever mutate in a way that suddenly causes them to be much more virulent. Pandemic flu viruses have a history of sometimes doing exactly that: mutating to be much more virulent than when they first emerged as a novel virus. Flu is never predictable, but the behavior of pandemic strains is even less predictable than that of seasonal strains.
So all communications that aim to “normalize” the pandemic to create the impression that it is “like the seasonal flu” are misleading, unless they also vividly dramatize the ways in which the pandemic and seasonal strains are different. Sometimes the misleading communications come from sources who don’t know they are misleading – local health officials or journalists who haven’t studied influenza or perused the relevant government statistics. But when the meme that the pandemic is “like the seasonal flu” comes from influenza experts who are compiling those government statistics, the communication is intended to mislead.
More often than not, the purpose of the misleading normalizing meme is to avoid frighening the public. We have written extensively about public health officials’ undue fear of public fear. (See “Fear of Fear: The Role of Fear in Preparedness … and Why It Terrifies Officials.”) When this type of over-reassurance is combined with efforts to get the public to take more than the usual precautions, it is a mixed message, likely to backfire in predictable ways:
- Some people who believe the reassuring half of the message will see no reason in take the precautions. (This is the outcome your comment focuses on.)
- Others will discount the reassuring half of the message, thereby losing some trust in the officials who issued the message – but will take the precautions.
- And still others will distrust both halves of the message, and seek unofficial sources of information in order to decide what to do. And we all know the range of unofficial sources that are out there in Blogville.
Other times – even more culpably – the purpose of misleading over-reassurance is to reduce the public’s demand for unavailable resources for coping with the problem at hand. For instance, public health officials in India routinely over-reassure their publics about various outbreaks for which they have inadequate vaccine or antibiotic supplies.
Regardless of why Italian officials are trying to convey the misimpression that the pandemic virus is just like a “normal” flu, it is bad risk communication. It will ultimately contribute to increased (and justified) mistrust of public health officials.
By the way, the public service announcement you link to also makes the misleading – but ridiculously common – assertion that the most important thing people can do to reduce their risk of catching the flu is to wash their hands. This message, too, is part of a pattern of over-reassurance. There is very little research evidence to support the notion that flu is significantly transmitted by virus on people’s hands, or that frequent hand-washing materially reduces flu risk.
Mandatory vaccination for health care workers
| name: | Ashley Conway | |
| Field: | Public health nurse | |
| Date: | October 23, 2009 | |
| Location: | New Jersey, U.S. |
comment:
Thank you for the September communication update on pandemic influenza. It was, as always, useful and insightful.
I am interested in knowing your thoughts about the New York State Health Department’s emergency regulation requiring seasonal and H1N1 influenza immunization for certain health care workers. Also, given your opinion about the questionable emphasis on seasonal flu vaccination, how you think the seasonal vaccine “shortage” impacts risk communication in the pandemic.
Peter responds:
Jody Lanard and I are firmly convinced that health care workers with patient contact should be vaccinated against both the pandemic flu and the seasonal flu. This isn’t just for the sake of their own health. It also helps protect patient health; people sick from other causes shouldn’t have their illness unnecessarily exacerbated by flu. And it helps reduce absenteeism at a time when the demands on hospitals and other health care workplaces are likely to be even greater than usual.
Given that employers, patients, and the public have a stake in the vaccination of health care workers, there is a pretty decent legal and ethical case for making vaccination mandatory.
Nonetheless, we’re against it. As risk communication consultants, we know that control is one of the most powerful of the outrage components. ![]() Coercion arouses outrage even when the coerced behavior itself doesn’t. And when the coerced behavior is something as personally upsetting as a medical intervention you have decided you don’t want, the outrage is likely to be extremely high. The resulting stress on health care workers’ morale, on labor-management relations, and on patient-provider relations is an awfully high price to pay.
Coercion arouses outrage even when the coerced behavior itself doesn’t. And when the coerced behavior is something as personally upsetting as a medical intervention you have decided you don’t want, the outrage is likely to be extremely high. The resulting stress on health care workers’ morale, on labor-management relations, and on patient-provider relations is an awfully high price to pay.
Moreover, mandatory vaccination will almost certainly increase the number of vaccinees who suspect that their future health problems are side-effects of the vaccine. An employer (or a government) that compels health care workers to get vaccinated can expect to face litigation not just about the legitimacy of the compulsion but also about specific health impacts attributed to the vaccine.
In “Talking about H1N1 Vaccination,” I argued that overselling flu vaccination was bound to backfire by arousing more outrage, more skepticism and resentment, and more psychogenic illness. The same is true – in spades – of requiring flu vaccination.
It’s not as if we were talking about a few idiosyncratic holdouts. In survey after survey, everywhere in the world, large percentages of health care workers have voiced their reluctance to get either flu shot. Though many health care workers have misunderstandings about flu and the flu vaccine (which they often communicate to patients), health care workers obviously are better informed and more experienced with regard to flu vaccination than the general public; and they have more reasons to get vaccinated than the general public. So it’s a very bad sign that flu vaccination proponents have failed to make their case in the minds of this crucial target audience.
The solution isn’t coercion. The solution is to figure out what vaccination proponents are doing wrong when they try to make their case. For at least part of the answer, see “Convincing Health Care Workers to Get a Flu Shot … Without the Hype.”
Ethicist George J. Annas recently wrote an excellent Newsday op-ed on this topic, “Don’t force medical pros to get H1N1 vaccine.” Annas’s op-ed helped persuade “revere” (the pseudonymous editor of the “Effect Measure” public health blog) to change his mind on the question. His October 5 post about why is worth reading, as are the comments that follow.
You also ask about the temporary shortage of seasonal flu vaccine in some places. As I’m sure you know, the seasonal flu vaccination campaign in the U.S. was pushed forward this year in hopes of getting it partly out of the way before the pandemic vaccination campaign got into gear. At the same time, the U.S. government asked manufacturers to interrupt their seasonal vaccine run in order to make pandemic vaccine, before completing seasonal vaccine production. So the early demand for seasonal vaccine (created by the government push) is outstripping the early supply in some places – though health officials are fairly sure that the supply will catch up, and in the end will probably exceed the demand as always.
In places where people are upset about the temporary shortage of seasonal flu vaccine, their worry and irritation should be validated as understandable. Public health officials should acknowledge their role in the shortage: They started early urging people to go get the seasonal vaccine, leading to some frustration when people tried to comply and found that there wasn’t enough vaccine for them yet because manufacturers were busy making pandemic vaccine instead.
Officials, especially local officials, should also emphasize much more frequently that so far there is almost no seasonal flu circulating in the U.S. So there is probably ample time to wait for the additional supply that’s coming.
And then officials should go further, acknowledging that there may be very little seasonal flu in the U.S. this year at all. If the pandemic H1N1 strain continues to circulate widely, it may out-compete and largely supplant the seasonal strains in our winter, as it did in most southern hemisphere countries during their winter. Officials are understandably reluctant to acknowledge this possibility, because they don’t want to discourage people from getting the seasonal vaccine. But the credibility of vaccination promotion – already in deep trouble – cannot afford the additional damage that will result if an aggressive seasonal vaccination campaign is followed by virtually no flu season at all, and officials are forced to concede belatedly that they always knew that was a distinct possibility.
The priority groups for seasonal vaccination and the priority groups for pandemic vaccination are different but overlapping. Health care workers are a priority group for both. So it makes sense to urge health care workers to get vaccinated as soon as they can with whichever vaccine is locally available first, and then to get the other one when it becomes available to them. And for health care workers who are reluctant to get both vaccines but willing to consider getting one or the other, it makes sense at this point to urge them to get the pandemic vaccine, since that helps protect against the flu virus that is widely circulating in the U.S. right now.
“Urge” – with evidence; with appeals to altruism and professionalism as well as self-interest; and with empathic acknowledgment of their concerns, their reservations, and their skepticism. Not require.
Research to prove that outrage management works
| name: | Andrew Macalister | |
| Field: | Communications consultant | |
| Date: | September 5, 2009 | |
| Location: | New Zealand |
comment:
I am interested to know if any research has been done to quantify changes in attitudes of members of the public to an outrage management situation, following the application of your risk communication principles – or some such “empirical” demonstration of the value of applying these risk communication principles.
Here is the background to my question:
New Zealand has a classic low hazard/high outrage debate that has been rumbling on for years – the aerial application of sodium monofluoroacetate (known as 1080) for pest control. A quick Google search will show up the tenor of the debate.
From 2002–2007 I was contracted by one of the two major 1080 users to establish a public consultation model for the aerial 1080 operations, in response to significant public opposition and operational delays. In doing so, I drew heavily on your risk communication principles.
With the consultation process in place in 2004, aerial operations were able to be planned and implemented on time, with the backlog cleared by 2005–06. In fact, only one operation between 2004 and 2007 generated strong public opposition. This was in stark contrast to the situation before I became involved, which was very inflamed.
During this time, I ended up managing the entire programme from 2005–2007. I resigned at the end of 2007 to resume some other projects, and unfortunately, since then, all the principles we put in place appear to have become eroded. Last year, the aerial programme erupted in a storm of acrimony and threats that hadn’t been seen since 2003.
I have the opportunity to put some research proposals up to my former client and, in the context of the above, believe it would be worth trying to set up a research project where we can tangibly demonstrate the value of good risk communication – such as by measuring attitudinal change before and after a risk communication intervention. I have talked to a couple of social scientists but am still struggling to define how we might set up such a research project. Hence my question – is there some existing research model that has been implemented in the past, which we could draw on?
Peter responds:
The “outrage factors” ![]() that lead people to experience a situation as high- or low-risk regardless of the actual hazard have been well-documented in research going back to the 1970s, especially the so-called “psychometric” research of Paul Slovic and colleagues. There are endless debates over how to measure the various factors. And it’s far from obvious how to combine them into a composite variable called “outrage” (or even whether it makes sense to do so). But nobody disputes that control, fairness, trust, dread, and the rest significantly affect the way people see risk. You can choose among a wide range of ways to measure these factors.
that lead people to experience a situation as high- or low-risk regardless of the actual hazard have been well-documented in research going back to the 1970s, especially the so-called “psychometric” research of Paul Slovic and colleagues. There are endless debates over how to measure the various factors. And it’s far from obvious how to combine them into a composite variable called “outrage” (or even whether it makes sense to do so). But nobody disputes that control, fairness, trust, dread, and the rest significantly affect the way people see risk. You can choose among a wide range of ways to measure these factors.
When we talk about measuring outrage, we can mean at least four different things.
- We can try to measure the outrage-provoking potential of the situation itself – the extent to which your organization shares control, acts fairly, builds trust, etc., and the extent to which it has done so in the past. This is the main focus of my “OUTRAGE Prediction & Management” software, for example (now downloadable without charge).
- We can try to measure people’s experience of the situation – the extent to which your stakeholders feel they have some control, are being treated fairly, can trust you to do the right thing, etc. This is what psychometric research does.
- We can try to measure the emotions and risk perceptions that these various outrage factors lead to – how frightened or angry people say they are, or how dangerous they say the situation is. These are often the outcome variables in social science research about risk.
- We can try to measure the behaviors that make outrage manifest – how many people join opposition organizations, sign petitions, participate in demonstrations, and the like. These are often the main concern of clients, but ideally outrage management aims to deter these behaviors rather than merely responding to them.
There has been much less research on what you want to study: the effectiveness of outrage management strategies ![]() . How is people’s outrage (in any or all of the four meanings listed above) affected by things like acknowledging your organization’s prior misbehavior and sharing control over how the situation is handled?
. How is people’s outrage (in any or all of the four meanings listed above) affected by things like acknowledging your organization’s prior misbehavior and sharing control over how the situation is handled?
To test the impact of various outrage management strategies you have to measure the outrage, of course. But that’s not the main problem.
The main problem is randomization. To find out how well various outrage management strategies work, you’d want to start out with lots of people facing some low-hazard, high-outrage risk controversy. You’d assign them randomly to receive different messages (apologetic or stonewalling, transparent or secretive, etc.), and then you’d see which groups ended up more or less outraged. Better yet, you’d have lots of different communities facing the same controversy, and you’d randomize them and treat them differently; that way you could explore the resulting group dynamics, not just individual reactions.
For obvious reasons, nobody does that. In the real world, it’s extremely difficult to randomize individuals – not to mention trying to randomize outraged individuals. It’s basically impossible to randomize communities, outraged or not. And no client would let you do it anyway. If you think stakeholders will calm down if you do X and get even more outraged if you do Y, your client isn’t about to authorize you to do X to half of them and Y to the other half in order to find out if you’re right.
So you’re left with three main research alternatives, none of them ideal.

Case studies.
Your comment mentions that you tried a combination of outrage management strategies with regard to aerial pesticide spraying in New Zealand, and together they worked pretty well. Then someone else took over, changed strategies, and stakeholder outrage went up. That’s a case study. It’s evidence – only anecdotal evidence, but evidence nonetheless. If some neutral third party were watching instead of you, it would be better evidence, less vulnerable to your bias that your way works best. But it would still be just an example, with no way to determine which of the things you did made the difference, or whether your outcome was typical or unique.
Despite the evidentiary weaknesses of case studies, most people find them persuasive – often more persuasive than rigorous quantitative proof. (Consider how a couple of neighborhood cancer stories can overpower a stack of epidemiology and toxicology reports.) In general, people learn best from their own successes and other people’s failures: “We did this and it worked. They did that and it backfired.” Learning from your own failures is tougher.
Case studies of outrage management failures are easy to find. When a community explodes in outrage, journalists will be there to cover the controversy, providing a rich (though not necessarily unbiased) source of data about what went wrong and why. Case studies of outrage management successes are much scarcer. Reporters don’t usually write stories about why people aren’t upset. And an organization that has done a good job of calming its stakeholders will rightly think twice before writing up its success, lest people feel manipulated and end up outraged about the successful effort to minimize their outrage. But there are some academic case studies available of good public engagement efforts regarding various controversies.

Focus groups and surveys.
A food industry client of mine has had several recalls in recent years, one of them serious. Consumer awareness of the recalls is high, as is food safety concern; some consumers have stuck with the company’s products anyway and some haven’t. The company needs to know how both groups feel about the company, its products, and its recalls; how they would react if there were yet another recall; and above all what they think of various food safety measures and messages the company is considering.
The best way to answer these questions is a series of focus groups, perhaps followed by a survey. Focus groups provide richer data, while surveys (with a random sample of the population of interest) provide more reliable data. So you use the former to suggest hypotheses and the latter to confirm them.
When it comes to testing possible outrage management approaches, survey methodology can be unwieldy, so organizations often rely on focus groups alone, figuring that if several focus groups have pretty much the same reaction, that’s the reaction you’d expect in a survey (and in the real world) as well. The trick is to make sure you’re testing your outrage management strategies in a realistic context. If you simply ask people which message they like better in the abstract, the one where you say everything’s fine or the one where you admit some screw-ups and promise to do better, a lot of them are probably going to prefer to be told that everything’s fine. But if you test the same two messages in the context of a “radio newscast” that quotes a range of sources, you’ll get a different response. Since the newscast covers other people talking about what you did wrong, the focus group is likely to respond better when you’re admitting the problem than when you’re denying or ignoring it.
Like case studies of successful campaigns, organizations’ focus groups are virtually always proprietary. Usually their surveys are too. And when organizations do intend to make their surveys public, they tend to ask different questions (and ask them differently), collecting ammunition rather than guidance.
Even surveys aren’t true experiments. You’re asking people how they responded when X happened, or you’re asking them how they think they would respond if X happened. That’s very different from making X happen to some randomly assigned people but not to others and watching how they actually respond.

-
Simulation experiments.
Although real-world outrage management experiments are unfeasible, if you’re willing to forgo the real world you can do a real experiment. Typical is a study I conducted in 1990 (back when I was an academic) with Paul Miller and Branden B. Johnson. We wrote hypothetical news stories about a perchloroethylene spill, systematically varying three factors: (a) the technical seriousness of the spill (the hazard); (b) the amount of technical information in the news story; and (c) the outrage in the news story – whether the government agency handling the cleanup sounded responsive or unresponsive, sympathetic or contemptuous, etc., and whether neighbors sounded frightened and angry or calm and impressed. Then we went door-to-door, asking people to read one story (chosen at random) and tell us how they felt about the spill. Our analysis was able to show that the outrage in the news stories affected people’s hazard perception more than five orders of magnitude of actual hazard.
For the details of this study and two others, see “Agency Communication, Community Outrage, and Perception of Risk: Three Simulation Experiments.” See also this index of some of my other research on outrage management.
From time to time risk communication scholars have done their own studies to test some of my outrage management principles and recommendations – sometimes with my involvement and sometimes without it. If you’re interested, check out the work of Lars-Erik Warg, Kjell Andersson, and colleagues at Örebro University (warning: most of it is in Swedish). Kenneth Lachlan and Patric Spence have also published several papers together (in English) on how to measure outrage and outrage management – see for example “Measuring Sandman’s Hazard and Outrage Model in Multiple Contexts.” I have some problems with how Lachlan and Spence define and operationalize my concepts, but probably I’m not the best judge of that.
There have been other outrage management studies over the years. Try searching in Google Scholar for Sandman + outrage + measurement.
A few years ago, Rob Folger at the University of Central Florida business school launched some research aimed at documenting whether companies could reduce stakeholder outrage by following my recommendations. I haven’t seen any publications yet – but you might want to contact him about his methodology (and why he gave up, if he did).
When they forgo real-world testing, simulation experiments forgo something else as well: the societal context. If you go door-to-door asking about hypothetical news stories, you can get a pretty decent idea of how isolated individuals tend to respond to news about a risk controversy. That’s on target for, say, a food manufacturer that has been through a few recalls. But in a hot local controversy, it’s not usually the response of isolated individuals that matters most. It’s the response of networked stakeholders – especially those who have gotten involved, gone to a few meetings, listened to the activists, and thought about becoming activists themselves. What does it take to get somebody like that to give you another chance? That’s probably the single most important outrage management question. Simulation experiments can’t answer it, nor can focus groups and surveys. You’re back to case studies.
Andrew responds:
Thanks very much for your reply. It has helped to clarify my own thinking on this.
Ultimately, I agree that real-world case studies which have not elicited negative behavioural responses would be the most persuasive argument for an outrage management strategy.
In a research context, however, it seems that a focus group approach before and after a real-world operation would be most useful. It is not a true experiment, but neither is most of the related field research undertaken in New Zealand in relation to the use of 1080. Conducting a focus group with willing participants from the affected community, and perhaps supplementing that with a small survey after the operation, would be relatively straightforward.
However, the additional problem I foresee is that in order to obtain the same participation before the operation commences, we would effectively be letting the cat out of the bag by alerting the respondents of the forthcoming operation in their area. That is unlikely to be acceptable to the agency.
Yet if we waited until the agency had made its initial advice of the operation, or even made the request for respondents’ input simultaneously, then I would feel that the baseline information was not truly valid. It would not be an accurate gauge of respondents’ attitudes before the operation, given that initial contact is so critical to shaping the response of the affected community.
Peter responds:
You’re right, of course, that focus groups and surveys have a Heisenberg effect: The measurement effort changes the thing you’re trying to measure.
It might make sense to use a panel approach – recurring focus groups with the same people. In a pre-1080 panel, you’d raise a variety of environmental issues, and ask generically how people think agencies ought to approach communities about controversial projects. The possibility of your someday using 1080 in the community would be just one of many items discussed, and unlikely to constitute a premature heads-up to the community.
Then, at about the same time as your first public contact about 1080 spraying, you’d reconvene the panel and get its early reactions. At the same time, you’d set up some additional focus groups with new people, as a control against the possibility that the panel had been sensitized and was therefore reacting differently than others in the community. As time went on, you’d continue to dialogue with your panel, and also to convene new groups.
This isn’t perfect either. For one thing, you'd need to be careful not to say anything in your first session with the panel that its members could see as misleading in hindsight. Maybe you should tell them straight out at the first session that you're considering a project that may be controversial, and that if it’s launched you’ll be seeking their counsel throughout the project – but this first session is to get broad answers to broad questions and you can’t reveal what the project is about until a later, more focused session.
Healthcare reform outrage
| Name: | Brad Ross |
| Field: | Corporate manager |
| Date: | August 31, 2009 |
| Location: | Arizona, U.S. |
comment:
It seems that the people in charge of developing the country’s healthcare policies and laws have done a great job of creating outrage. I see so many of the issues you talk about in this debate/debacle. Seems like the first thing all of the politicians should do is bring you in to teach them a thing or two about outrage management.
Perhaps they could start by saying they are sorry that they fouled up the process. Then they should think about the outrage factors such as control, fairness, process, and dread to change the way the debate is being managed.
Any chance you are getting involved in this to help the process along? I think we need your help.
Peter responds:
I agree with you that an outrage management perspective could have helped – and could still help – to get a decent healthcare reform bill passed. And I think your suggestion to start with an apology for having mishandled the debate is excellent!
I wish I could get involved – even though I’m awfully busy with pandemic communication right now. But no, nobody in the administration (or anywhere else) has approached me about this issue. Other than my recent Guestbook entry on the healthcare “town hall meetings,” I haven’t worked on it at all.
Empathy, Les Havens, and Elvin Semrad
| Name: | David Mobley |
| Field: | Project Director, Elvin Semrad Archive |
| Date: | August 29, 2009 |
| Email: | DMobley184@comcast.net |
| Location: | Massachusetts, U.S. |
comment:
With regard to your excellent article on empathy and its afterword by your wife in 2007, there is a wonderful cassette tape still around in which Les Havens expresses with great compassion what Semrad had taught him. (Originally it was to do with helping in extremis suicidal patients to want to survive.)
OED traces “to share” back to the shearing of sheep – that is to say, taking action which lightens the load to the benefit of both parties. All the accumulated worries and fears which so burden a person invite frustration, rage and hate. The caregiver has to demonstrate a vivid, deep contact with all that, before the other person can experience some measure of relief that he is not alone with it, it can be “sheared.” In some cases this involves dramatics, in other cases a deft touch of perspective.
I think Les would enjoy very much many of your phrasings of volatile situations because the right performative has remained a staple of his style. The former student of Dr. Havens, Elissa Ely, continues his good work in her commentaries with NPR and the Boston Globe.
Peter responds:
Thank you for the wonderful connection between “sharing” and “shearing.”
You wrote to this Guestbook once before after my wife Jody Lanard and I mentioned Elvin Semrad in a website column on “Talking about Dead Bodies.” The “Empathy in Risk Communication“ column never mentions Semrad, but leans heavily on his former student, Leston Havens.
Your comment that “Les would enjoy very much many of your phrasings of volatile situations because the right performative has remained a staple of his style” is particularly heart-warming to Jody, who is a former student of Dr. Havens (and a psychiatry residency-mate of Elissa Ely). Out of shyness, Jody missed several chances to show Les the impact his teaching has had on our work. It is wonderful to get indirect validation from you.
We would love to listen to the Havens/Semrad tape, if you have a copy you could send us.
Agricultural risk communication and human health
| Name: | Amy Delgado |
| Field: | Veterinary epidemiologist |
| Date: | August 29, 2009 |
| Email: | Amy.delgado@iica.int |
| Location: | Costa Rica |
comment:
I have greatly enjoyed and valued your comments on risk communication and disease control and prevention, and I have found them to be incredibly useful in many settings. However, one area that I would love to hear your thoughts on is communicating with the agricultural producer.
Perhaps this falls under the area of segmenting your audience, but I feel that this is a group that is consistently under-targeted or poorly targeted in official communication efforts. Unfortunately, this is a group whose participation, voluntary or otherwise, is usually essential to effective disease detection and control. With so many diseases able to transmit between people and animals, agricultural producers are often the front line of our detection and defense systems. In addition, they often bear the brunt of the expense for disease mitigation measures simply for the “common good,” with little or no financial benefits.
As an example, the swine flu pandemic cost U.S. swine producers millions of dollars and decimated the swine industry in many countries simply because the name “swine flu” was circulated early on, despite no evidence of a link with swine or pork. Now as our curiosity regarding the source and spread of influenza viruses takes a new direction, it will not be long before agricultural health agencies are asking producers to accept disease surveillance programs, enhanced biosecurity requirements, and possibly increased testing requirements for the “safety” of their products.
How do you feel that the communication messages for this group should differ from those for the general public (keeping in mind that they are the general public as well, since they still have to make decisions about what they eat)? Have you been involved in any efforts to develop or plan communication strategies for this audience? Many thanks!
Peter responds:
Your comment addresses how officials communicate with agricultural producers. Your real concern, if I’m reading you right, is how human health officials communicate with owners of farms and agricultural companies.
After I address your issue, I can’t resist turning the tables. You’re unhappy about the way human health officials address agricultural concerns. I take your point. But I’m at least as unhappy about the way farm organizations and agricultural agencies address human health concerns.
When human health people talk about agriculture
As you suggest, the connections between human health and agriculture are becoming more and more obvious, more and more politically loaded, and more and more burdensome on agricultural producers. The main connection of interest used to be foodborne illnesses – and that issue, too, is hotter today than it has been for some years. But we have also entered a new age of infectious diseases. Since many of the highest-profile infectious diseases (including bird flu and swine flu) are transmissible between animals and humans, and since some lower-profile animal-to-human diseases are prevalent (salmonella, campylobacter) or on the rise (Listeria), a whole new cast of characters is paying attention to farm practices … and asking for a variety of agricultural changes aimed at protecting human health.
Your contention is that the health officials pursuing these changes need the cooperation (“voluntary or otherwise,” as you say) of agricultural producers. But, you say, they’re not communicating well with agricultural producers. They’re not talking to farmers enough; they’re not listening to farmers enough; when they do talk or listen, they’re not doing so empathically enough.
Although I haven’t made a thorough study of how health officials communicate about agriculture and how they communicate with farmers, I think you’re almost certainly right. One sign that you’re right is the systematically scanty communication between health agencies and agricultural agencies, even within the same government, about pandemic influenza. My wife Jody Lanard and I have given a large number of pandemic communication seminars (usually separately). The health department sponsoring the event rarely invites participants from its sister agriculture department, even when we have vehemently urged that ag officials be invited. When there is an ag person in the room, he or she is usually the only ag person in the room – and his or her comments often have an understandably beleaguered tone.
If health department communicators aren’t in frequent contact with ag department communicators, and if health department technical people aren’t in frequent contact with ag department technical people, what are the odds that health department messaging aimed at farmers is going to show a decent understanding of what those farmers are up against? And what are the odds that health department recommendations about agricultural practices will be actionable, or that farmers will be inclined to act on them?
So you end up (for example) with public health campaigns requiring farmers in rural Asian villages with nearby bird flu outbreaks to exterminate their healthy flocks, without acknowledging that this constitutes an economic disaster for the farmers and the villages. As I wrote in a December 2006 Guestbook answer:
My wife Jody Lanard and I have done some work (Jody more than I) with international agencies and Asian governments wishing to encourage farmers to cooperate with culls. They often try to claim that an H5N1 outbreak is a serious threat to the health of the farmer and his family. This is simply false. Bird-to-human transmission of H5N1 remains difficult; only a few hundred cases have cropped up in the face of millions of opportunities. Interacting with sick birds is nowhere near as dangerous to the farmer as losing his livelihood. And of course there is no “business case” whatever for a farmer whose birds are healthy to destroy his own livelihood in order to create a cordon sanitaire and stop the spread of infection. That’s wise for the world at large, for reasons of poultry industry prosperity as well as pandemic prevention. But it is surely a net loss – a catastrophe, in fact – for the farmer, his family, and his village. We have advised clients to say exactly that. (It’s not a secret; claims to the contrary are transparently false.) Of course what makes most sense is for the developed world to subsidize compensation to developing world farmers, whose sacrifice helps to protect us all. If compensation isn’t in the cards, there are two other options: appeals to altruism and coercion. Dishonest claims that the farmer ought to want to cull his flock undermine altruism and add insult to the injury of coercion.
Consider in this context the recent discovery in Chile that turkeys can catch the human pandemic H1N1 swine flu virus, and the evidence from Manitoba that pigs (unsurprisingly) catch that virus quite easily (from humans or from each other). In humans, pandemic H1N1 swine flu spreads easily but is very mild (so far). Panzootic H5N1 bird flu, on the other hand, is incredibly deadly to humans, but only rarely spreads from birds to people, and almost never spreads from one person to another (so far). Every epidemiologist’s nightmare is a reassortment of the highly lethal H5N1 virus with the currently pandemic H1N1 virus, which could potentially produce a new pandemic virus with the transmissibility of swine flu and the virulence of bird flu.
So we really don’t want any human, bird, or pig to have both diseases at the same time – and if that does happen we want to know about it as fast as possible, so we can take appropriate steps to reduce the odds that a reassorted virus (if there is one) could escape. We may be entering a period in which bird flu is widespread in birds and sometimes infects pigs and humans, while swine flu is widespread in pigs and humans and sometimes infects birds. If so, we will need the best communications we can manage between public health officials and agricultural producers – worldwide.
Profoundly unempathic bird flu risk communication in Asian villages helped sensitize me to the problem of health officials who either don’t understand or don’t acknowledge agricultural realities. I haven’t paid as much attention as I should to the same problem in the developed world, including the U.S. Even for me, health risk communication and agricultural risk communication have been in separate silos. I will try to do better.
When agriculture people talk about human health
Now let me turn the tables. I have been working for several decades trying to help both industry and government improve their understanding of risk communication principles. Some industries and some arms of government have tended to be quick learners. Others have lagged behind. Agriculture has consistently been among the laggards.
Here are just three of my complaints about how agriculture people talk about human health risk. I welcome your response – and the response of other readers – and maybe eventually I will write something longer (and more thought-through) on agricultural risk communication.
Food safety communication.
With regard to the most obvious intersection of agriculture and human health, food safety, both the ag industry and ag regulators have a long record of over-reassurance. I’m not qualified to judge whether the level of foodborne illness in developed countries like the U.S. ought to be lower than it is – whether there are cost-effective measures that should be implemented to reduce it. But it is a fundamental risk communication blunder to keep telling the public that food is “safe,” rather than teaching the public that pathogens are everywhere, that foodborne illness can be reduced but not eliminated, that further improvements in food safety will come at a cost, and that opinions differ on which improvements are worth the cost. The public is primed to overreact to periodic newsworthy recalls largely because we measure food safety performance against the yardstick industry and government have jointly implied: zero tolerance of foodborne illness. And when a specific overreaction occurs, companies and regulators either ridicule that reaction or pretend to share it; what they don’t do – and should – is apologize for having created unrealistic expectations in the first place.
Conflict of interest.
Note how I keep talking about “the ag industry and ag regulators” as one entity. That’s how they come across. At least in the U.S., the same government department (USDA) looks after the interests of farmers and polices the behavior of farmers. I understand that these sorts of conflicts of interest are nearly universal and very difficult to avoid. (It is a similar conflict, for example, that health departments promote vaccination, administer vaccination programs, and monitor for vaccination side-effects.) But in agriculture departments, promotion is the main responsibility, and regulation too often looks like an afterthought. This contributes to what I see as the regulators’ genuine tendency to understate and perhaps under-regulate agriculture-related health problems. At the very least, it contributes to the public perception (which I share) that regulators cannot be trusted to take agriculture-related health problems seriously enough, and cannot be trusted to be promptly and completely honest when such problems arise. When the regulator is also a cheerleader, we rationally mistrust the regulator – even if it is actually doing a good job. And when the industry looks largely unregulated, we rationally mistrust the industry, even if it is actually doing a good job too.
Cover-up.
When agricultural producers have contamination problems or disease outbreaks, they naturally try hard to get them under control. But they don’t necessarily reveal them promptly. There is a long history of farmers getting caught trying to cover up early signs of contamination or disease in order not to hurt the market for their crops or animals. We therefore have to assume a parallel history of successful cover-ups. Once again, public mistrust is one of the outcomes. And once again, regulators are often complicit. I don’t mean to suggest that regulators or even farmers routinely cover up problems that they consider significant threats to human health. I think they routinely cover up problems (or facts) that they consider trivial threats to human health, and that they worry the public may see differently. See for example the long column Jody Lanard and I wrote in 2004 on “Misleading toward the Truth: The U.S. Department of Agriculture Mishandles Mad Cow Risk Communication.” Similarly, I have watched as state agriculture departments in the U.S. suppressed some information about bird flu outbreaks in birds, fearing that the public might jump to the false conclusion that local birds were infected with the scary kind of H5N1 … and stop buying locally produced poultry. For instance, when New Jersey reported that a local bird flu outbreak was not caused by “N1,” Jody and I had to file a Freedom of Information Act request to learn what the “H” was, after months of government stonewalling.
An industry perceived as more trustworthy, and as better regulated, would likely have paid a lower price when one of its products was associated with the name of a novel human disease than an industry that people perceive as covering up problems and in bed with regulators. And in the specific case of “swine flu,” the ag industry might have recovered faster if it had shown some empathic understanding of the public’s initial reaction, instead of insulting people by insisting their temporary aversion to pork was “irrational” or “hysterical.”
Amy responds:
Thank you so much your response. I feel that you have captured some truly critical points, and I greatly appreciate the organization that you have brought to the issue. I find it very helpful to examine communication for producers and the public by human health agencies and animal health agencies separately, while, unreasonable as it may seem, I think I have had them combined in my head (in one silo, so to speak).
I would have to say in all fairness that I am unhappy with risk communication and agriculture in general, but my thoughts resonate most strongly with the latter half of your comments – perhaps because I feel that I have the most opportunity to make an impact there. I do not work for a regulatory agency. IICA is a branch of the Organization of American States, an institute dedicated to technical cooperation and the provision of technical expertise. However, we interact with agricultural departments from almost every country in our hemisphere.
I am a relatively new student of the risk communication field. My first introduction to it was actually at a crisis communication workshop you led in Guelph, Canada several years ago relating to food safety. So my admitted bias favors your “Risk = Hazard + Outrage” framework, which formed the foundation from which I have continued to learn about risk communication.
I just have a few thoughts regarding your response that I thought I might share. I certainly understand the point that you make regarding the apparent conflict of interest inherent in U.S. regulatory structure, and I would also agree that in general, agricultural agencies do a terrible job of communicating about human health risks. How agricultural regulators are seen by the public and the resulting loss of trust is a serious issue indeed.
At the same time, I think there is a second problem that probably contributes to the first, which is how ag regulators communicate with the agricultural community. Here is where I think discussing communication based on the perception that ag regulators and the ag industry are the same may limit the progress that can be made. Only by understanding that ag regulators, the ag industry, and the agricultural community are all different, can we begin to make some progress on how we communicate with agricultural producers. (And I think the same could be said for how human health agencies communicate with producers.)
Agricultural producers are a pretty diverse bunch. Within the U.S., for example, the vast majority of our food is produced by a small percentage of companies (which could be construed as “the industry” in terms of political clout). However, there are still hundreds of thousands of other producers who keep just a few head of cattle, or have a small flock of birds in their backyard merely for the enjoyment of having animals in their lives or for a few extra bucks or for a myriad of other reasons. These producers rarely see themselves as part of the “industry” and have traditionally been ignored by animal and human health agencies alike. (You may remember when animal health agencies suddenly “discovered” live bird markets in the U.S. and decided that maybe they should be inspected. The same could be said for fighting cocks, gaming pheasants, etc.)
Communication with these producers needs to embrace the idea that people may raise animals or grow crops for reasons other than economic gain and their goals may be different than trying to maximize production. Some people’s cows have names. Some people can trace the lineage of their livestock back to their great-grandfather’s herd. Some people only see their cows once a year when they round them up to take to the sale barn. I am sure that the same could be said for people who keep backyard poultry. Animal health agencies may be reluctant to commit what limited resources they have to this segment of producers who actually contribute so little to the nation’s food supply (or GDP). However, from a disease or risk perspective, they are just as important as any large producer, and in the case of avian influenza, perhaps much more so.
I think that the danger of defining the ag industry on the basis of political influence or organization has been sharply highlighted by the recent struggle to promote (or force through) a national animal identification system (NAIS). The ability to individually identify and trace animals during disease outbreaks is a standard criterion for effective emergency response, and the USDA has continually recognized the need for traceability in the agricultural sector. However, not surprisingly, minimal progress was made on an identification system until it was felt that “industry” supported the idea. This “industry” support came about as a consequence of several large-scale disease outbreaks in other countries and, following 9/11, the subsequent focus on food defense.
However, once the time came for NAIS to be implemented, producers and animal owners came out of the woodwork to oppose the system. It became apparent quickly that the agricultural system, when taken as a whole, was outraged at the proposed NAIS plans. Now it may be that agricultural producers are just ardently opposed to regulation. (I don’t think that would be a stretch for any industry.) However, after interviewing numerous cattle producers in Texas, I learned that many were not opposed to the regulation itself or the need for traceability in the food supply. What upset them were all the issues that typically come into play when you think of outrage – fairness, distribution of risks and rewards, concerns over personal privacy, etc. Small producers in particular are not able to separate their agricultural enterprise from their personal life. They are one and the same. They were in essence being asked to register their house with the federal government, so that the government could show up at any moment and kill their livestock if the government felt it was needed. The entire process of trying to develop, promote, and implement an animal identification system was a complete risk communication disaster, in part because it was done with the idea that if animal health agencies could persuade “industry” than everything would be fine.
(Disclosure: The cattle producer interviews were conducted as part of a USDA / Cooperative State Research, Extension, and Education Service-funded grant exploring the social context of highly contagious disease control in Texas.)
So I hope that perhaps I could persuade you to expand your framework to include both how agricultural agencies talk about human health risks and how agricultural agencies talk to the agricultural community. We have so much work to do in both areas.
I deeply appreciate your taking the time to respond to my questions, and I look forward to reading anything else you might have to say on the subject. Thank you again for your wonderful website and all the time and work that go into it. I’ll be sharing your post with everyone I can get to read it!
Coping with the outrage at healthcare reform “town hall meetings”
| name: | Catherine Roth | |
| Field: | Healthcare technology | |
| Date: | August 17, 2009 | |
| Location: | California, U.S. |
comment:
Given the madness that has infected the Congressional recess town hall meetings (talk about Outrage with a capital O), what is your advice for President Obama and members of Congress?
Are there techniques for dealing with outraged public behavior in a group setting – where the anger of a few generates mob-like reactions on both “sides”? Or is this just an impossible situation that cannot be salvaged, only avoided?
Peter responds:
As a rule, politicians are not very good at what I call outrage management: talking to people who are hostile, suspicious, or upset. Politicians’ customary communication tasks are trying to arouse the fervor of dedicated supporters and trying to inculcate mild support in people who care very little one way or the other. The first task calls for one-sided exhortations; the second calls for one-sided sound bites. Neither calls for the basic strategies of outrage management: acknowledging the other side’s sound arguments, acknowledging your side’s past missteps and current problems, giving your critics the credit they typically deserve for forcing you to do better, etc.
For a while I thought President Obama was an exception, able to talk empathically about his opponents in ways that felt right to the opponents’ constituents even when he was unable to win over the opponents themselves. During the campaign, he showed a stunning ability to summarize his opponents’ arguments cogently and respectfully, demonstrating that he really did “get” what they were trying to tell him. I thought he had an instinct for outrage management, not just for public relations. (He is still untested in crisis communication.)
If he really did have an instinct for outrage management, he seems to have lost it – I hope temporarily – in his advocacy of his healthcare reform policies. I don’t want to belabor this point, which has been widely commented on by others and seems pretty obvious to me. But here are three examples:
- The President and his administration promised that they could expand and improve healthcare while cutting its cost. When the Congressional Budget Office predicted otherwise, his reaction was to discipline the CBO, not to rethink the claim. The President hasn’t just continued to insist that he can accomplish this miracle of medical loaves-and-fishes. Maybe he can. What is especially discouraging to me is his reaction to those who doubt that he can; he has been reluctant to concede that it’s possible to have such doubts without being a fool, a villain, or even an opponent of healthcare reform.
- The accusations of opponents are usually a mix of valid grievances, exaggerated complaints with a germ of truth, and crap. Especially if you’re feeling as outraged as your opponents are, it’s awfully tempting to ignore the first two and focus on rebutting the crap. And it’s awfully tempting to pretend the first two are crap. It seems to me that the President and his administration have done some of that, trashing the foolish arguments against his plan instead of respectfully addressing the sounder arguments. “Any time you’re tempted to label and dismiss an opponent’s half-lie,” I tell my clients, “try admitting the half that’s true instead.”
- The President and his administration planned a series of recess “town hall meetings” to drum up support for his healthcare reform bill. Inevitably and appropriately, opponents of the bill saw the meetings as their best opportunity to drum up opposition as well. That’s democracy. I’m not sure what the President found so objectionable. That doubters came to the meetings? That they spoke up? That they weren’t always courteous? I haven’t watched tapes of the meetings or read the transcripts, but I’m guessing a good outrage manager would have allowed opponents to vent, restrained supporters from venting back, validated some of the opponents’ concerns, and even identified some lessons from those concerns that might usefully be incorporated into the bill. That doesn’t seem to be what usually happened.
There is a generic problem here that goes to the core of your question.
Some controversies are battles between two outraged, polarized extremes. One side is fighting angrily for X; the other side is fighting just as angrily for Y. Each side focuses on arousing its own partisans and attracting neutrals; neither side makes much effort to win over the other.
Other controversies aren’t that symmetrical. One side – typically the one with less institutional power – is battling to topple the status quo. Its key strategy is to arouse outrage, as intensely and broadly as it can. The other side is playing defense, trying to lessen the intensity and breadth of stakeholder outrage, to calm the waters, to negotiate a peace rather than win the war. Controversies between activists and government or between activists and companies typically take this form. Only the activists are trying to arouse outrage; the company or government agency is trying to manage outrage in hopes of reducing it.
Risk controversies are typically like that too. The side arguing that X is intolerably dangerous wants as much outrage as it can get. The side arguing that X is acceptably safe wants as little outrage as it can get. In my terms, this is a fight between precaution advocacy and outrage management, between those who wish to warn and those who wish to reassure. Because the strategies of precaution advocacy and outrage management are so different, it’s not a symmetrical fight. The side trying to warn can afford to exaggerate and be rude (within reason), while the side trying to reassure must listen respectfully to the opposition’s arguments and acknowledge the ways in which those arguments have merit.
When you’re trying to arouse outrage, in short, you can treat the other side as your enemy. When you’re trying to ameliorate outrage, you must treat the other side as a respected critic from whose criticisms you intend to learn.
The healthcare policy debate could have shaped up as a battle over the acceptability of the current U.S. healthcare system. Advocates of change would have tried to muster as much outrage as they could about the millions of uninsured Americans, the screwed-up incentives that reward doctors for performing unnecessary procedures, the ability of insurers to cherry-pick customers and refuse to cover preexisting conditions, the danger that people can lose their insurance when they lose their jobs, the ever-rising cost of healthcare for the individual and the society, the hatefulness and incomprehensibility of insurance company paperwork, the immense profitability of the for-profit health insurance industry, the fact that other developed countries produce better health outcomes at much lower cost, etc. Defenders of the status quo would have tried to calm the waters and negotiate a mutually respectful compromise that changed as little as they could manage.
But as it turns out, the debate has shaped up not as a battle over the acceptability of the status quo but as a battle over the acceptability of the Obama reform package. Advocates of change have found themselves trying to negotiate a mutually respectful compromise that changes as much as they can manage, while defenders of the status quo get to make the outrage-arousing arguments: that we don’t want the government controlling our healthcare choices; that the Obama plan will put private health insurance out of business; that we’ll end up socializing yet another hunk of the economy; that the new bureaucracy will put the country even further into debt; that rationing, euthanasia, and who knows what other evils lie buried in the fine print.
Why did it turn out that way? I’m not certain, but here are some possible reasons:
- A lot of Americans don’t actually hate the healthcare they have. They’re afraid of losing what they have – a fear that is at least as strong when they contemplate the Obama reform package as when they contemplate the current system. Even those who do hate the current system may worry that they’ll hate the new system more.
- More generally, what psychologist Daniel Kahneman calls “loss aversion” is in play here. For most people, keeping what you already have is far more highly valued than getting something better; that’s why “double or nothing” isn’t a popular bet. This is a “risk heuristic” that every change movement comes up against. “What if our efforts to make things better end up making things worse?”
- We have been hearing for decades that America’s healthcare system is broken. Yet it keeps lumbering on. Although we speak of the healthcare “crisis,” for most Americans it feels more like a chronic problem we ought to tinker with than an emergency we must urgently redesign from the ground up. A lot of people would happily accept medication for our ailing healthcare system, but they’re leery of major surgery.
- It’s hard for the President of the United States with a commanding majority in both houses of Congress to play the outraged underdog. And Obama’s persona, his not-so-secret weapon, is cool, not heat.
It is possible that the Obama team could have seized the outraged position – played offense instead of defense. It is possible that they still could.
But I doubt it. I think this is the metaphorical battlefield they’re stuck with: an establishment juggernaut deploying rational, wonky arguments to change the U.S. healthcare system, up against a guerilla movement that finds the proposed changes terrifying and infuriating. The irony here is extraordinary. The left certainly sees itself as David in this fight, and sees the insurance companies as Goliath. But most of the country sees it the other way. The change agents, the insurgents, have become the establishment. Instead of attacking the status quo, they are stuck defending their proposed replacement for it.
Given that that’s how things have shaped up, opponents of the healthcare reform package are strategically wise to try to arouse as much outrage as they can on their side. And supporters of the reform package are strategically unwise to join them in polarizing the debate, instead of trying to manage the outrage downward. So far, in short, opponents are handling the town hall meetings skillfully, and President Obama’s forces are mishandling those meetings badly.
So how do you handle a town hall meeting that’s packed with outraged opponents? The protocol for outrage management at meetings is clear:
- Let your opponents vent. Listen hard. Take notes. Don’t interrupt, except possibly to echo a point or ask a clarifying question.
- If some opponents are going overboard in their criticisms, let them. Even defend their right to be rude and repetitive. Such fanatic excesses are likely to offend the moderates on their own side. Trust that if you refrain from heavy-handed policing of the debate, social pressure from the crowd will keep the meeting from getting out of hand. (Of course you must do what it takes to ensure everybody’s physical safety.)
- Try to make sure moderate critics also get a chance to speak. Don’t worry much about giving your supporters a chance to speak – especially your more fanatic supporters, who are likely to do you more harm than good. You’re here to listen to critics and address their concerns, not to argue back.
- Don’t respond prematurely. The first few times you’re asked to respond, demur on the grounds that not everybody has been heard yet and you’re learning a great deal from what people are saying. Wait to speak until the room has united behind the premise that it’s your turn – until the more moderate skeptics have shushed the determined opponents and demanded that they give you a chance to speak.
- When it’s finally your turn, start by summarizing what you think you have heard. Check to make sure you heard it right. Don’t give your main talking points. Summarize your critics’ talking points instead, respectfully and accurately.
- Then focus on the valid points that have been made against your position. Don’t validate points you don’t consider valid – but don’t take too much time rebutting them either. Disagree briefly and then let them slide, devoting yourself instead to conceding that, yes, X, Y, and Z are real problems with your proposal.
- Explore interactively what might be done about X, Y, and Z to make your proposal a better proposal.
This outrage management meeting protocol can usually accomplish what it’s designed to accomplish: It lowers the emotional intensity of your critics; it convinces your moderate critics that you really understand their concerns; it shows them that you are willing to listen to criticism (even extreme criticism), and that there are grounds for further dialogue in hopes of coming up with a revised proposal they can live with.
But there are things it doesn’t accomplish – three in particular.
First, it doesn’t give you much chance to arouse the fervor of your supporters. In fact, good outrage management almost always irritates your supporters, who don’t like to see you turning the other cheek, responding respectfully to people who aren’t respectful to you, acknowledging the other side’s good arguments when you could have rebutted the other side’s crap instead. Cooling opposition tempers and whipping up fervid support are antithetical goals; it’s awfully hard to do both at the same meeting. If arousing your supporters will do you more good than calming your critics, that’s a pretty good reason for diverging from the outrage management strategy.
Second, it doesn’t give you much chance to rebut totally fallacious arguments being deployed against you. This is a tough call. If you spend a lot of time trying to prove that X is an idiotic argument, you pay one set of prices: focusing everybody on X and turning up the flames of debate when you wanted to turn them down. If you leave X unrebutted, or only briefly rebutted, you pay a different set of prices: giving some people the impression that you must not have a satisfactory answer to X. If you think a rebuttal will change a lot of minds on an issue that’s doing you real harm, that’s a pretty good reason for diverging from the outrage management strategy.
Third, it doesn’t give you much chance to woo neutrals – newcomers who haven’t given the issue much attention so far and don’t really know where they stand. Acknowledging the other side’s good arguments leaves these newcomers thinking the other side has some pretty good arguments. Rebutting the other side’s crap leaves the newcomers thinking the issue is complicated and it’s hard to figure out who’s right. The best way to woo marginally attentive neutrals is usually to present your side’s good arguments, rather than responding to what the other side has been saying (which marginally attentive neutrals may well not have heard). If you think you need to get uninvolved people to end up weakly on your side instead of weakly on the other side, that’s a pretty good reason for diverging from the outrage management strategy.
Of course there are mixed strategies that try to split the difference. But a town hall meeting is only so long. The sound bites television crews take away from the meeting are a lot shorter still. You can split the difference, but you can’t do all of everything.
It does seem to me that the Democrats’ advance work for some of these town hall meetings was less than sterling. Perhaps in an effort to avoid accusations of filling the room with supporters who would throw lobs instead of brickbats, it looks like the Obama team filled the room with hostile opponents instead. I’m a big believer in outrage management, but even I would have aimed for a more balanced crowd than some of the town hall meetings ended up with – Senator Specter’s near Pittsburgh, for example.
Still, whatever crowd you have at the meeting itself, your real audience is the rest of the country – a mix of critics and skeptics, supporters, and marginally interested newcomers. If you do a good job of ameliorating the outrage of critics and skeptics, you’re likely to irritate your own supporters, and you may well lose ground with the marginally interested newcomers. If you do a good job of inspiring your supporters and winning over the newcomers, you’re almost certainly going to further outrage the critics and skeptics.
In short, the price you pay for doing good outrage management is supporters who are disappointed that you’re not standing tall for the team and newcomers who learn that the other side does actually have some valid points. The price you pay for selling your strengths to your own supporters and the newcomers is further alienation of those critics and skeptics.
Do you want to polarize the battle and win (or lose)? Or do you want to search for a compromise, a middle ground that everybody but the extremists on both sides can live with?
I think President Obama should want to search for a middle ground on healthcare policy. I also think he was searching for a middle ground on healthcare policy. But his opponents tried to polarize the battle instead, a strategically sound decision on their part – and they sucked him into doing likewise. So now we have mutually antagonistic speakers at town hall meetings, and mutually antagonistic sound bites about the town hall meetings, with each side accusing the other of intransigence and dishonesty.
President Obama and his spokespeople need to decide what posture or postures they want to emphasize in the healthcare policy debate:
- respectfully listening to their critics and validating their valid arguments;
- passionately arousing their supporters;
- angrily rebutting opposition arguments they consider unfair; or
- calmly laying out the affirmative case for healthcare reform.
My strongest impression is that the Obama team has been doing too little of the first, forfeiting what has been one of the President’s greatest strengths as a leader. I think maybe it has been doing too much of the second and third. I’m not sure about the fourth – it may be doing too little of that too.
Role of faith organizations in pandemic preparedness / response
| Name: | Dan Dyck |
| Field: | Director of Communications, Mennonite Church Canada |
| Date: | August 13, 2009 |
| Location: | Canada |
comment:
As a communications practitioner with involvement in pandemic preparedness communication, I’ve been following your posts with a great deal of interest.
Something I’ve not seen much of in the wide variety of pandemic prep information is content focused on the vital role faith groups can play in all phases of a pandemic. Here in Canada, the government’s public health agency has recognized the role faith groups can play in the event of a pandemic. After all, even fast food chains cannot rival the many, varied, and isolated locations in which congregations find themselves.
Faith groups have some unique advantages besides their number of “outlets” and “locations”: Each faith group’s facility could potentially serve as a triage centre; each faith group can exercise influence in communicating a variety of health topics, from hygiene to caring for shut-ins, to its adherents; faith groups traditionally are a great source of volunteers in times of crisis. And of course spiritual care is a huge component for individuals in times of illness and personal crisis.
To this end my denomination has developed a web site: www.churchpandemicresources.ca. While the content is geared to those of the Christian faith, there is nonetheless information that can be put to use by people of other faith backgrounds as well.
What are you hearing about the role of faith groups in pandemic preparedness?
I hope you can spend some time on this website – and perhaps you might find the concept compelling enough to write a post about it on your site sometime.
Peter responds:
I certainly agree that faith groups are ideal for provoking and facilitating communal pandemic preparedness and pandemic coping. The only comparably decentralized nonprofit institution is the public schools, which are much more constrained by their government connections than churches, synagogues, and mosques are.
Among many contributions churches etc. could make, one that’s dear to my heart is neighborhood stockpiling of food, medications, and other supplies. People who feel they can’t maintain their own stockpiles for reasons of space or finances might collaborate on a church-run stockpile. I’d be happier, I think, to see a church stockpiling for (and with) everyone in its neighborhood rather than congregants only – but any communal stockpile increases people’s feeling that we’re all in this together while decreasing the number of unprepared individual households.
I have also talked about the possibility that churches could develop rosters for a pandemic volunteer survivor corps. If the pandemic becomes more pervasive (as seems likely) and if it turns more severe (anybody’s guess), there will be a need for lay volunteers – especially volunteers who have recovered from the flu and are probably immune. (I say “probably” because the virus can drift, or the original influenza-like illness might not have been H1N1 after all.) Volunteers could wash linens at hospitals, deliver food to flu victims, replace absentees in essential jobs, etc. I’d love to see churches building databases now of people who are ready to be deployed if they get swine flu and then recover (as well as those who have had swine flu and recovered already) – people who have already registered their skill sets and signed their informed consent forms.
Although I haven’t made any sort of careful study of how faith communities are responding to the pandemic risk, my sense is that the response has been supportive but tepid. Religious leaders have generally been more than willing to cooperate if asked, but not especially interested in leading the way. The few church-related pandemic websites I have seen tend to feature links to government sites, and they generally replicate government advice.
This includes a tendency to accept unquestioningly even the very debatable things governments are saying. Thus, since the arrival of H1N1 the U.S. and Canadian governments have been reluctant to urge people to stockpile food and other supplies against the possibility of supply line disruptions and resulting shortages – and so churches have expressed little interest in fostering or coordinating such stockpiles. Governments have grossly overestimated the value of hand-washing – and church sites have replicated the overstatement. (Hand-washing is certainly harmless in communities with plenty of clean water, but it is probably only marginally useful, since most experts believe flu is transmitted mainly by droplets and not often by hand contact, and since the flu virus lives only a very short time on the hand anyway.)
Based on my very brief perusal of www.churchpandemicresources.ca, these observations seem to hold true for that site as well.
I have also noted that religious leaders around the world have sometimes responded to community fears (or official fears) by constraining religious practices in order to prevent transmission of the virus. For example, some churches have temporarily abandoned the kiss of peace or the sacrament of communion. Such measures are certainly appropriate when a virulent and highly transmissible pathogen is widespread in a community. They may well turn out useful in the months ahead. But they have quite often been implemented prematurely, in communities where there wasn’t yet much swine flu and without seeming to notice that swine flu is quite mild so far. I have mixed feelings about the impact of such premature precautions – whether they are useful rehearsals for the tougher times that may be coming or over-alarming signals about the severity of the current situation. Judging from what I have seen of church communications about why they are doing what they’re doing, the latter seems likelier to me.
These are all tentative impressions. If I decide to take you up on your suggestion to write about what faith institutions are doing and what they could be doing, I would need to try to confirm or disconfirm these impressions – and learn a lot more about how faith institutions are responding and planning to respond to H1N1. Toward that end, I would welcome any further information you might want to send my way.
I should add that whether or not the pandemic turns more severe, the experts do expect it to become more pervasive. As pandemic “waves” roll from place to place, there will probably be periods of a few weeks to a few months during which the number of sick people in a community will exceed the capacity of that community’s healthcare system. The place for very sick people will still be hospitals, or perhaps special influenza care centers. But the place for people with mild cases will be home, cared for by their family, friends, or neighbors. I would be shocked if religious organizations did not play a major role in pandemic homecare, whether they prepare for it now or not.
Dan responds:
You have made several valid and insightful observations about the religious community’s response.
And I agree to some extent that these comments are also applicable to www.churchpandemicresources.ca. The objective of our site was originally to build a case for WHY people of faith must respond to a pandemic – the same spiritual imperative that explains why we respond to hurricanes, earthquakes, floods, etc. We also wanted to be useful beyond that, and serve people by providing links to information that already exists rather than duplicating it. Still, your counsel about blindly following government in its recommendations, and the timing of communication, is well advised.
That said, I’m grateful for the fresh insights you offer about things churches can do – some of which I, at least, had not considered before. Clearly we are all on a learning curve as this event progresses, and as we connect more with others and learn from one another.
The importance of telling people about pandemic flu precautions
| name: | Knut Ihlen Tønsberg | |
| Field: | Public relations | |
| Date: | August 12, 2009 | |
| Email: | 123bratt (at) gmail.com | |
| Location: | Norway |
comment:
Regarding your “Three-Legged Stool of Pandemic Messaging,” I think your fourth message should be included, what people should do themselves.
A mild influenza is also serious, as you have mentioned earlier. We can show solidarity with the vulnerable groups (pregnant women, etc.) by trying to slow the spread of the disease until we have the vaccine.
I understand your point that the experts do not think taking precautions will have much effect. But if sick people stay home for seven days, if people all wash their hands and cover their coughs, etc., it could at least be worth trying, even according to their own theory.
The message that pandemic influenza is “mild” depends on what you compare it to. That was an appropriate message in the beginning of May, to tell people that the virus is milder than originally anticipated. But why now? I think the facts we should highlight instead of mildness are: (1) the vulnerable groups, (2) the symptoms (fever, etc.), and (3) the importance of getting Tamiflu within 48 hours after feeling sick (especially for vulnerable groups).
After highlighting these three facts our message should be: Everybody can do a little to help slow the flu. And by doing so are we showing solidarity with the vulnerable groups until a vaccine is available.
If we don’t tell people to help slow the flu, then if there are fewer deaths than anticipated, the health authorities will be blamed for misleading the public, not be credited for their good work.
The message to the health sector should be to take this “mild” virus more seriously than other mild diseases and be quick to provide medicine and care.
The Canadian website “FightFlu” has the best message I have seen so far.
What do you think? Things might look different from the other side of the Atlantic; Europe is some weeks behind the United States in flu developments.
Peter responds:
You make a good case that it’s important to tell people what they can do to reduce their chances of getting and spreading the flu (pandemic or otherwise), and what they should do if they think they have it. Among the reasons why this is worth doing (some of which you mention):
- Flu precautions do work to some extent. People who wear masks, wash their hands, avoid crowds, and the like are a little less likely to get the flu. People who do these things and stay home when they’re sick are a little less likely to give the flu to others.
- Even if one-quarter to one-half of us still wind up catching H1N1 by the end of the pandemic, spreading out the concentration of illness is a worthwhile goal too. If fewer people are sick at the same time, absenteeism problems and the burden on doctors and hospitals will be smaller.
- Taking steps to avoid getting the flu is especially important for people who are in vulnerable groups, such as pregnant women. If the rest of us also take precautions, we’re not only helping protect those people; we’re also showing solidarity with their need to protect themselves. (I hadn’t thought much before about your solidarity point, but it certainly underscores that “we’re all in this together” – one of my crisis communication mantras.)
- People who know the symptoms of influenza and know that antivirals need to be taken ASAP after the onset of symptoms are less likely to suffer from complications, require hospitalization, or even die. It may be difficult to reduce the pervasiveness of the pandemic, but we can reduce its severity.
- When we take flu precautions seriously, we are telling ourselves that flu is serious. That is, precautionary behavior tends to lead to precautionary attitudes – which then lead to more precautionary behavior. I’ll bet that people who are convinced to cover their coughs, wash their hands, wear masks in crowded places, etc., will be likelier to go get vaccinated once a vaccine is available. (Some commentators worry that precaution-taking might lead to “a false sense of security.” I think Leon Festinger’s theory of “cognitive dissonance” plays a much bigger role. The more pandemic precautions we have taken, the more we are likely to take.)
- People who are really upset about the pandemic find it easier to bear their fears when they have things they can do to feel less powerless. This group – those who are alarmed rather than complacent – is likely to grow as the pandemic becomes more pervasive, especially if it also becomes more virulent. Recommending useless precautions raises unacceptable ethical and credibility problems, in my judgment – but finding precautions we can ethically and credibly recommend is important.
You mention another possible benefit of precaution messaging – your judgment that it will give health authorities some cover from accusations of overreacting if the pandemic turns out very mild and not very disruptive. Perhaps you’re right that people who have taken precautions themselves may decide the pandemic fizzled (if it fizzles) because of those precautions, not because the authorities were overreacting in the first place. But I wouldn’t count on it. I suspect people who were persuaded to take precautions may feel all the more aggrieved if they later decide those precautions weren’t necessary.
But you have convinced me: Precaution messaging is important. I would make sure to stress that the precautions we’re recommending will help only a little, that the pandemic is expected to be pervasive no matter how conscientiously we wash our hands and cover our coughs. But the precautions are worth talking about. So my three-legged stool now has four legs. Now it’s a chair.
Please note: Quite apart from the pandemic precautions we are discussing here, I have always strongly recommended preparedness in case the pandemic takes a turn for the worse. The plea for preparedness is at the heart of the third message – possible future severity – in my three-legged stool. It is also the main thrust of my first column on swine flu, published on April 29: “The Swine Flu Crisis: The Government Is Preparing for the Worst While Hoping for the Best – It Needs to Tell the Public to Do the Same Thing!”
Judging from your comments, you’re not convinced that the comparative mildness of the virus (so far) deserves to be a core message. We certainly agree that mildness is relative. People need to know that even a “mild” pandemic can overcrowd hospitals, shut down schools, and kill significant numbers of people. I have written elsewhere about the dangers of overstating the “mildness meme.”
Even so, I think comparative mildness needs to be one leg of the stool/chair. Here’s why:
- It’s true. The available evidence suggests that so far the pandemic has a lower case fatality rate than the seasonal flu. That could change – and possible future severity is a key message too. But pretending the pandemic is more severe than it is not only risks accusations of hype; it makes those accusations accurate.
- Credibility is at stake. Pandemic messaging needs to prepare people for the worst. But it also needs to prepare people for a 1968-like pandemic that’s not such a big deal. Health authorities shouldn’t stake their credibility on a big-deal pandemic. They will need that credibility for the next pandemic if this one turns out to be a dud.
- A lot of people are skeptical, believing that the pandemic has been hyped from the outset. Convincing them to take it seriously requires, at a minimum, conceding explicitly that (so far) it’s nowhere near as bad as 1918 and nowhere near as bad as it looked at first.
- A lot of people are frightened. That’s hard to realize in the U.S., where complacency is the main problem. Maybe complacency is the main problem in Norway as well. But think about the U.K. and Argentina, where fear (though not panic) is widespread. And think about all those countries that have had only a handful of deaths so far (or even none), where many people imagine that H1N1 is a death sentence that has to be “contained” at all costs.
- Effective pandemic messaging should be balanced. My three-legged stool has good news (it’s pretty mild so far) and bad news (it’s probably going to be pervasive and it might get more severe). Leaving out the good news – or the bad news! – unbalances the messaging and tips over the stool.
Am I late urging people to prepare for a possibly severe pandemic?
| Name: | Gaudia Ray |
| Field: | Volunteer activist |
| Date: | July 12, 2009 |
| Location: | Nevada, U.S. |
comment:
So, it’s your turn to reach the same conclusion I did, that government officials are irresponsible as they refuse to embrace the risk of the severity of pandemic flu, and do the one thing that would help, [urge people to ] stockpile the essential non-comestibles.
I admire that you’ve stood up this time and not cooperated with or joined (yet), as contractors, the establishment. They may yet buy you off. For the sake of your message now, I hope that’s not the case.
I’m glad you’re doing this. I [will] spread the word re this article.
Peter responds:
I am grateful for your support for my most recent Swine Flu Pandemic Communication Update, “Why Pandemic Complacency Isn’t Okay.”
I have been urging government to urge people to prepare for a possibly severe pandemic for several years now. See for example, “The Flu Pandemic Preparedness Snowball,” written in October 2005. Or read the full range of my pandemic articles, columns, and interviews, all listed in “Pandemic Flu and Other Infectious Diseases Index.” Jody and I wrote a l-o-n-g four part column in March 2007 on “What to Say When a Pandemic Looks Imminent” largely in order to help officials realize that they’d better start saying those things before a pandemic looks imminent. As we wrote in Part 4:
The best way to make your pre-crisis communications more candid, more alarming, and more realistic is to spend some time planning your crisis communications. Then go back and ask yourself what changes in your pre-crisis messaging would pay dividends if the crisis were ever to materialize.
But I understand that some in the pandemic preparedness community see me as having betrayed the preparedness cause from time to time, especially when I voiced the view that periods of low public interest weren’t propitious times to push hard. (See “What do I think about the controversy in the pandemic prep community about my role and my integrity?”) So I accept your tentative welcome back in the spirit in which I think it was intended.
Using public health concerns and public health departments to sell climate change action
| Name: | Kathy Dervin |
| Field: | Public health |
| Date: | July 5, 2009 |
| Location: | California, U.S. |
comment:
I am looking at ways in which state and local health departments can add their voices to the chorus working on climate protection. Climate change is clearly a threat to current and future public health around the world, the greatest challenge ever, perhaps.
Public messaging and educational efforts that focus on health (personal health, community health, family health, international health, and the health of future generations) may be a powerful vehicle to stress the urgency of dealing with climate change (both mitigation and adaptation).
I’m just wondering about your take on the messenger. Do you think health professionals (medical and public health spokespeople, local and state health departments, health voluntary organizations, even your family doctor) stand a good chance of constructing and delivering the kinds of messages that may help people:
- Understand a little bit more of the climate change situation and see what we can do to offset the worst of climate change effects (by translating highly technical issues into simpler but serious messages that have an action orientation).
- Be more inclined to take some action (if connected to health issues and health spokespeople).
- Develop more the human face of climate change, climate change effects, and climate actions people can take.
I’m trying to figure out what can be done to develop roles that health/public health leaders and professionals and community health advocates can play. How can they take whatever credibility they may have and use it strategically (but sensitively) in message campaigns of various sorts? There is urgency in this effort and a lot of complexity. Do you believe health professionals can help cut through this with a focus on human-scale issues and actions?
Peter responds:
As I’m sure you know already, health concerns are much more personally meaningful to most people than environmental concerns. Environmental activists and environmental regulators cottoned onto this early; as far back as the 1980s, “environmental health” was a major focus of environmental activism and regulatory activity – sufficiently so to be controversial within the environmental community, where there were complaints that the emphasis on short-term human health concerns was sapping attention and resources from longer-term issues, habitat issues, etc. It’s arguable that action on climate change might have come more quickly if environmentalism hadn’t taken the human health route so one-sidedly.
The focus on environmental health was also controversial within the public health community, which worried that it was sapping attention and resources from more urgent health issues. Most environmental problems rank pretty low compared to other threats to human health, especially in the short-term. Environmental activists and environmental regulators routinely anguish over risks that are thought to kill a handful of hypothetical people per million people exposed; anything that killed one in ten thousand would be a huge environmental health problem. Compare that to the numbers for diabetes, HIV, obesity, etc. When environmental health concerns are housed in a state health department, they tend to look pretty minor compared to other health concerns; when they’re housed in an environmental protection department, they tend to look important compared to other environmental concerns.
So there is psychological merit (and justice) in using health concerns to motivate climate change action. And of course there is an ever-increasing literature (which you know a lot better than I do) to suggest that the connection is legitimate. It might be easier to arouse people about the prospect of malaria and dengue becoming widespread in California than about the prospect of polar bears disappearing from the Arctic.
That said, the messenger problem is tougher. Public health agencies have been eviscerated in the past few decades (another fact you know better than I do). And public health as a concept has declined as well, I think. So now we have agencies without the resources (or morale? or expertise?) to take on a big issue that isn’t obviously their issue (as, say, flu, MRSA, AIDS, and TB are), and a public that would be initially perplexed to hear from them on that issue … and perhaps perplexed to hear from them at all.
The decline of communicable diseases as a focus of personal and parental worry is part of why the resources of public health agencies and the public’s support for the public health concept have both declined. Maybe the H1N1 pandemic, the AIDS pandemic, and the rise of antibiotic resistance will help.
So you have a cluster of problems to overcome as you try to mobilize public health agencies on behalf of climate change:
- The agencies are underfunded and overworked.
- The agencies may see themselves as mostly about infectious diseases.
- The public has little understanding of public health, low interest in it, and low expectations for it.
- The public may also see public health (to the extent they see it at all) as mostly about infectious diseases.
- The public sees infectious diseases as a problem that has pretty much been solved.
Here’s the paradox. Most people care more about their health and their family’s health than they do about the environment. Health is vivid and urgent; the environment is abstract. Since a health threat is more emotionally arousing than an environmental threat, and since climate change is both, it makes sense to stress its health-related aspects. But most people see environmental issues as calling for government action and collective societal action, whereas they see health issues as profoundly personal, between them and their doctors. “Health” is hot but “public health” is not. (There is no comparable distinction between “environment” and “public environment.”) So it may be going against the grain to make health – public health, collective health – a core basis for policy change and social change to address global warming.
In general, bootstrapping doesn’t work all that well in communication. Are we using climate change to sell public health or using public health to sell climate change? Both are arousing much less public concern than they should. What do we gain when we yoke two undernourished issues? Can they feed each other somehow?
All that notwithstanding, I’d like to see you develop a campaign that yoked climate change, infectious diseases, and public health: “If you think swine flu is bad, wait till you get your first taste of dengue and malaria, right here in the good old USA, thanks to climate change….” Yoking climate change to other aspects of public health is also worth trying.
Kathy responds:
I see what you mean about health departments being eviscerated and being perceived in a certain way. But we are also involved in asthma, healthy homes, the fresh foods movement, city and urban planning (health and the built environment – where you live has a whole lot to do with how healthy you are), etc. And we do a whole lot on chronic disease, some of which clearly links physical activity (walking and biking) and reducing vehicle miles traveled. Did you know that green building-efficiency standards are not the same as HUD’s healthy home standards – and in fact by making houses more efficient you are going to create indoor air quality problems that will lead to (or aggravate) more health problems?
Our health department has one communicable disease nurse (with others pulled in as necessary – and nearly everyone pulled in for H1N1!). But we have 30 staff doing health promotion/chronic disease prevention work – some of which can relate to climate issues in one way or the other – that I agree is probably not obvious to most in the community.
Walking (as a way of life) can help reduce your risk of diabetes and obesity and it can help reduce greenhouse gases, but only if you live somewhere where walking is safe and, better yet, enjoyable (trees, bike paths). We are trying to find ways to stress these “co-benefits.” It will take a culture change, but that’s what happened with smoking in California.
Plus public health doctors, nurses, etc. can help add their voices/credibility to the climate change effort, raising health issues like heat. Also we work a lot with low-income-community advocates who are also working on environmental justice and climate justice.
Washington State is just developing a big climate change campaign. I am trying to find out more about this. We cannot figure out, with all that’s going on in California under AB 32 (the California Global Warming Solutions Act), why we have not yet come up with powerful messaging to accompany all the work we’re doing. Of course, there is this little problem with our budget. The states are way ahead of the feds at this point – but is the public really informed and being engaged?
Pandemic prioritizing: Vulnerable people versus essential people
| name: | “Avalanche” | |
| Field: | Clear-thinking survivalist (or not?) | |
| Date: | July 5, 2009 | |
| Location: | Georgia, U.S. |
comment:
In your piece on “Is Swine Flu ‘Mild’? Are We Safe If We Have No ‘Underlying Conditions’?” you have the following sentence, with which I must take exception:
It tells policymakers that they should prioritize people with the listed conditions when it comes to allocating scarce resources, such as antivirals and vaccines.
I realize you’re writing about the still “mild” swine flu that is circling the globe at warp speed; however I think I see that same less than complete meta-message that I see elsewhere (pretty much everywhere, it seems, except on a few hard-core survivalist forums). The underlying (unconsidered? unaddressed?) premise to such a statement seems to be that scarce resources should be allocated on the basis of the health of a (of any) person, and not on the needs of society.
Try to reconcile the above with the kinds of societal disruptions you (barely) touched on in your most recent column, “Containment as Signal: Swine Flu Risk Miscommunication”:
Will it get bad enough to shut down factories, schools, and essential services due to absenteeism? Again, nobody knows. But some local ambulance companies have already reported limited service because of swine flu absenteeism. And today’s just-in-time supply chains are fragile. If too many coal miners or railroad employees call in sick with the swine flu at the same time, coal-fired power plants could run out of fuel and major cities could go dark. If the factories in developing countries that manufacture surgical masks and generic drugs can’t operate or can’t ship, U.S. hospitals and pharmacies could find themselves with empty shelves. These are just “tip of the iceberg” examples of possible supply chain problems in our globalized just-in-time economy.
Then prioritizing the people who have underlying conditions, without considering whether or not those people are necessary to the continuation of society, is the wrong choice for policymakers to make! You point out in many of your recent writings that important “teachable moments” are being missed by governments and health officials, and that false or misleading reassurances are, intentionally or unintentionally, being given to the public(s). Yet, in my eyes, here’s a truly fundamental (and vitally important) teachable moment, and I think you have not tried to use it to teach – or perhaps, in teaching another lesson, you’re leaving out a huge portion of a necessary lesson – that triage will be different if this H1N1 plays swap with, say, H5N1 (out there in Asia where they’re both wandering around).
Yes, the need to “prioritize people with the listed conditions when it comes to allocating scarce resources” is a next big step – but the harsh reality of prioritizing people with those conditions is that they will need to be prioritized at least one priority level below people such as these:
- healthcare workers (and administrative folks who order medical supplies, and hospital janitors who clean facilities and sterilize equipment, and whomever else the hospitals need to keep running)
- police officers and firefighters (and their dispatchers, and their vehicle maintenance folks?)
- electricity generation plant workers (and the folks who allocate and control power on the grid, and line repairers)
- sewage treatment plant workers and potable water suppliers
- food delivery system workers (not just truck drivers – who will offload the trucks and stock the shelves, and what about supermarket checkout clerks?)
So some 30-year-old man with diabetes, or a kidney-dialysis-requiring mother of two, or 16-year-old twins with asthma, or any of a thousand – a million! – permutations of “people with the listed conditions” must be prioritized below, say, an emergency room nurse with no such conditions, a firefighter in excellent health, and the guy who runs the filtration system at the local sewage plant (at all the hundreds and hundreds of sewage treatment plants there are in this country!), whose work is necessary to keep cholera at bay!
This is one of the hardest concepts that must be dealt with in this (or the future severe) pandemic. And everyone seems to gloss right over it, because it’s uncomfortable and requires considerations that we don’t feel good about. Peter, for all your excellent work in trying to get people to understand what’s coming (now or later, this virus or another), you, too, seem to want to leave out the really horrendous decisions that will have to be made – and if we don’t discuss them now, we’re sure not going to have any luck discussing them once the truly deadly pandemic begins.
Are you leaving out these horrific considerations because you think they distract from the (smaller) teachable moment(s) you currently have? Or are you avoiding them, like so many others, because they are horrific and asking people to face them is more likely to throw them into denial than help them realize that this WILL be the new normal, and they’ll have to face it at some point? Or, as I think when I’m feeling especially despairing, will the folks in charge actually prioritize “scarce resources, such as antivirals and vaccines” to the 30-year-old man with diabetes, and the kidney-dialysis-requiring mother of two, and the 16-year-old twins with asthma, and just ignore the likelihood of chaos following on the faltering of society’s infrastructure?
Peter responds:
You’re right that if conditions get bad essential people ought to have a higher priority than vulnerable people. You’re right that there ought to be a lot more discussion about this prioritization dilemma before the need actually arises. And you’re right that a universal queasiness makes us all reluctant to have that discussion – political leaders and public health officials for sure, and maybe me too.
I did touch on the issue in the 2006 column on Tamiflu stockpiling I wrote with my wife and colleague Jody Lanard. Here’s what we said then:
If a pandemic comes soon – and if Tamiflu helps – governments will face difficult choices about how best to ration their limited supplies. As noted above, two main rationing strategies are in contention:
- Use the Tamiflu to treat the most vulnerable flu victims, those you think are likeliest to die if untreated….
- Use it to protect and treat the people we most need to keep healthy in a severe pandemic….
It is debatable which uses for Tamiflu should have top priority. And it’s a debate that ought to happen now, before the pandemic, with broad public involvement. Although most experts favor the second strategy, especially if the pandemic is severe, different national governments (and different local governments) may well make different rationing decisions.
But if you are neither especially vulnerable nor especially useful, you’re not going to be on anybody’s list….
There is quite a large (and growing) professional literature on “pandemic ethics,” in which the allocation of scarce medical resources (vaccines, antivirals, ventilators, etc.) is often the dominant issue. And just about every government’s pandemic plan includes some kind of priority list. As a rule, I think, the lists do prioritize “essential” people ahead of “vulnerable” ones – as you recommend. Their definitions of who’s essential tend to be pretty narrow, though. Healthcare workers are likely to be higher on the list than, say, power plant workers. And people with irreplaceable professional and technical skills tend to be higher on the list than people whose jobs are just as essential but whose educations are less rarefied, like truck drivers and cops.
Here’s how the U.S. Department of Health and Human Services talks about pandemic vaccine allocation ![]() :
:
One of the most important findings of the working group analysis, and the strongest communication from the public and stakeholder meetings, was that there is no single, overriding objective for pandemic vaccination and no single target group to protect at the exclusion of others. Rather, there are several important objectives and, thus, vaccine should be allocated simultaneously to several groups. Each of the meetings came to the same conclusions about which program objectives are most important:
- Protecting those who are essential to the pandemic response and provide care for persons who are ill,
- Protecting those who maintain essential community services,
- Protecting children, and
- Protecting workers who are at greater risk of infection due to their job.
In addition to these, working group discussions highlighted the important Federal objective of maintaining homeland and national security.
Most government (and corporate) pandemic plans were drawn up with a severe H5N1 pandemic in the backs of the authors’ minds. This has clearly influenced thinking on prioritization of scarce medical supplies – even though prioritization discussions usually acknowledge that much depends on how severe the pandemic turns out to be. The HHS guidance document, for example, points out that “it is important that plans are flexible as the guidance may be modified based on the status of vaccine technology, the characteristics of pandemic illness, and risk groups for severe disease – factors that will remain unknown until a pandemic actually occurs.”
Now a pandemic has actually occurred, and it’s mild so far – not as mild as most Americans imagine, but certainly milder than “severe pandemic” prioritization recommendations envisioned.
Think this through with me.
First imagine the nightmare scenario: a pandemic that infects one-third to one-half the world population (as is typical of flu pandemics) and kills roughly 60% of the people it infects (a much, much higher death rate than any flu pandemic we know of, but the actual death rate so far of non-pandemic H5N1). Obviously, the very survival of society as we know it is threatened. Just as obviously, anybody who gets the flu and isn’t treated stands a very good chance of dying – so decisions about how to allocate scarce medical resources stand a very good chance of determining who lives and who dies. Conclusion: Use your vaccines and antivirals to save the lives of the people most essential to keeping things going. Prioritize the essential people, not the vulnerable ones.
Now imagine a pandemic that kills nearly nobody – one in ten thousand, say, about an order of magnitude less severe than the seasonal flu. There may still be some supply chain problems caused by absenteeism if lots of people are sick at the same time, but “keeping things going” isn’t the desperate problem it is in the first scenario. Moreover, only the most vulnerable people are likely to die if they don’t get medical help; everybody else will recover anyway. So if you give your scarce vaccine or antiviral dose to a healthy person in an essential occupation, a very sick person in a less essential occupation may die. If you give it to the vulnerable person, they’ll probably both pull through. Conclusion: Prioritize the vulnerable people, not the essential ones.
Nobody can predict whether the H1N1 pandemic of 2009 will turn out closer to my first scenario or my second. It certainly looks more like the second scenario so far.
There has never been a pandemic of any disease as bad as the first scenario. The Black Death (plague) pandemic of 1347–1351 “killed an estimated 30–50% ![]() of the European populations affected.” The 1918 Spanish Flu pandemic killed about 2.5% of those it infected, enough to make it the worst flu pandemic we know about.
of the European populations affected.” The 1918 Spanish Flu pandemic killed about 2.5% of those it infected, enough to make it the worst flu pandemic we know about.
So far, the swine flu pandemic is a piker by comparison. In the U.S., the CDC guesstimates that more than a million Americans have had swine flu already – and only 127 of them died. That’s just 1.27 deaths in every ten thousand cases, compared to roughly one in a thousand for the seasonal flu. If the H1N1 pandemic is really eight times milder than the seasonal flu, and if it stays that way, prioritizing the vulnerable is certainly the way to go. But it’s early days yet. These preliminary figures could be mistaken, or the virus could get more virulent in the months ahead. The 1918 pandemic started mild too.
So we should plan for a range of severity scenarios. We should try to figure out how to distinguish a pandemic that’s severe enough to prioritize essential workers from one that’s mild enough to prioritize vulnerable patients. We should concentrate on developing mixed priority plans (like the HHS vaccine allocation guidance document I quoted earlier) for intermediate pandemic scenarios.
And as you stress, we should get past our discomfort and try to get the public thinking about these questions with us. Despite some excellent small-scale public engagement projects over the past few years, the general public has not been encouraged to think about this issue at all.
Is right now a good teachable moment for the pandemic prioritization dilemma? I’m not sure.
On the one hand, I am convinced that most Americans are pretty complacent about this swine flu pandemic. It’s hard to get them to take it seriously, hard to get them to prepare, hard to get them to consider that it might turn more virulent. So maybe we need to make progress on those fronts first.
On the other hand, “whose life should we save” is a pretty compelling question; it’s intrinsically more interesting than how many cans of tuna to stockpile. So maybe talking about how to prioritize access to scarce medical resources in a pandemic emergency is a good way to introduce the reality that we may – or may not – end up faced with just such an emergency.
I do despair of convincing political leaders and public health officials to launch that sort of dialogue with the public. A few years ago, when we faced no pandemic at all but were worried that we might be facing a severe H5N1 pandemic soon, U.S. officials were interested in telling the public to prepare … and even in asking the public’s opinions on the ethical dilemma of prioritizing access to scarce medical resources in a pandemic emergency.
Now we do face a pandemic. It’s H1N1 rather than H5N1, and it’s pretty mild so far. But it could get worse. And H5N1 still looms. The risk of a severe pandemic has to be higher today when we face a mild one than it was a few years ago when we faced none at all. Although political leaders and public health officials are taking that risk ever more seriously themselves, they are much less interested in asking the public to take it seriously than they were a few years ago.
I haven’t had much success convincing U.S. leaders and officials to talk about public pandemic preparedness again. I haven’t had much success getting them to focus more on addressing (widespread) swine flu complacency than on preventing (virtually nonexistent) swine flu panic. I doubt it’ll help to urge them to explain whose life they plan to save if and when people start dying in droves and there isn’t nearly enough vaccine or Tamiflu to go around.
But at least I should talk about it here.
Do I really think people should have Tamiflu on hand? Yes.
| Name: | Debbie |
| Field: | Citizen |
| Date: | June 23, 2009 |
| Location: | Ohio, U.S. |
comment:
This is in regard to the individual who was “trying to get Tamiflu….”
Here are a couple of questions that come to mind. Can I get a prescription for morphine “just in case” I get hurt? Can I add to the list of drug-resistant microbes by taking the wrong medication for an illness?
And what really surprised me was your response!
Peter responds:
You’re right that there are big problems associated with making it too easy for people to get access to abusable painkillers like morphine – though many patients with recurring back problems and the like do in fact keep narcotics on hand (with their doctors’ okay) for moments of need. Tamiflu isn’t similarly abusable. It gives the user no pleasure and often leads to nausea; nobody would take it who didn’t genuinely think s/he had the flu.
As for resistance, Jody Lanard and I wrote about that in our original 2006 column on “The Dilemma of Personal Tamiflu Stockpiling.” As we wrote then, you can’t create Tamiflu-resistant flu virus by using Tamiflu when there’s no flu virus present; you simply waste the Tamiflu. Resistance is a risk when Tamiflu is used to treat an actual flu case. So it’s debatable whether to prescribe Tamiflu when the patient’s case is mild and the patient has no other medical complications … or when the patient has been exposed to flu but has no symptoms (and may have an asymptomatic case) … or when the patient is likely to stop using the Tamiflu before it’s done (again, likeliest with a mild or asymptomatic case). It’s sometimes hard to decide when the risk of resistance might outweigh the benefit of using the drug – but in cases where people mistakenly think they have the flu, the risk of resistance is zero.
As we wrote in our 2006 column, Jody and I continue to think that it makes sense for people to stockpile a drug (like Tamiflu) that might save their lives if they need it, when they know in advance they’re likely to have a hard time getting it after the need arises. The “dilemma” our column title referred to was the dilemma of a possible shortage. We argued that every individual is better off having some Tamiflu on hand, but the society as a whole might be better off if the limited supply of Tamiflu were allocated by some central authority.
When we wrote the column, bird flu concern was at its height and the Tamiflu supply was genuinely limited. Because the demand (individual plus government) exceeded the supply, Roche increased its manufacturing capacity, and by early 2007 the supply overtook the demand. As time went on, the public’s bird flu fears subsided, most U.S. states decided to buy less Tamiflu than the federal government had allocated for them, and Roche took note of the declining demand and shuttered one of its Tamiflu plants. So there was no more dilemma, as I wrote in an August 2007 Guestbook entry entitled “Tamiflu redux.”
Anyone who stockpiled Tamiflu between February 2007 and the emergence of swine flu in April 2009 wasn’t hoarding a scarce medication; he or she was contributing to the market demand for a medication in oversupply.
Swine flu changed the situation yet again. Many governments (including the U.S. government) have mobilized their Tamiflu stockpiles, often using the drug not just to treat people with swine flu (or some flu) but also to protect (and reassure) their contacts who don’t have any flu so far – classmates, airplane seatmates, etc. Meanwhile, the amount of Tamiflu available from pharmacies is at a low ebb, in response to the previously low demand – so the new demand has led to shortages.
For obvious reasons, Roche is now manufacturing Tamiflu as fast as it can. But swine flu is now officially a pandemic, probably destined to infect billions of people worldwide over the next couple of years. There is now once again a shortage of the drug, not an excess. If the novel H1N1 swine flu virus doesn’t develop Tamiflu resistance, that will probably remain the case for some time to come.
People who try to get Tamiflu now face a practical problem; people who find a way to get it now face an ethical dilemma. But people who got it over the past few years faced neither.
Readers pondering the Tamiflu dilemma might want to check out this article from the June 15, 2009 Salt Lake Tribune. According to the story, a Utah woman got sick with flu-like symptoms after caring for her mother, who had already tested positive for flu and been treated with Tamiflu. But the women herself tested negative for flu twice. Although false negatives are quite common with the rapid flu test, the doctors treating her refused her requests for Tamiflu. She died.
Outrage management for receptionists and operators
| name: | Marilyn | |
| Field: | Mining industry public relations | |
| Date: | June 16, 2009 | |
| Location: | Utah, U.S. |
comment:
I have been asked to provide some training and guidance for the receptionists and operators at all the front desks and main phone numbers of our company, who may encounter a variety of passionate members of the public or passionate employees and their families, on a number of topics, either by phone or in person.
Do you have a set of tips for dealing with people who are concerned or angry, deescalating a situation, etc., that I could use with these people, who are our day-to-day public interface?
Peter responds:
As you know, I do a lot of outrage management seminars for senior executives, public affairs people, ES&H people, HR people, etc. But it’s a rare company that asks me to train its receptionists and telephone operators.
That has always struck me as strange, since these frontline people are often your first point of contact with outraged stakeholders, whether they’re employees, neighbors, or customers.
Even more importantly, these frontline people are typically your first point of contact with stakeholders who aren’t systematically outraged, only temporarily upset – so far. I would wager that a lot of dedicated activists have launched their activist careers after an unsatisfying contact with a receptionist or an operator.
Picture this. Somebody storms into an office or calls an executive, pretty steamed about a problem that has just arisen. The visitor or caller isn’t necessarily courteous; s/he’s upset, after all, and not happy to be dealing with an “underling” instead of the boss. The receptionist or operator who’s stuck coping with the situation has no training for it, and responds to the discourtesy by becoming irritated or evasive. And that’s the moment a long-term critic is born.
The principles of outrage management are the same, of course, whether you’re the CEO or the switchboard operator. See my Outrage Management Index for a list of relevant columns, articles, and Guestbook entries. A good place to start might be the “Laundry List of 50 Outrage Reducers” – a pretty decent overview of a lot of strategies, all laid out quickly rather than in the excruciating detail of a lot of my other writing.
What’s unique about outrage management for receptionists and operators? They’re usually talking to people who are trying to get past them to somebody “important.”
Assuming you’re asking your receptionists and operators to backstop the visit or call, rather than pass the person on, the protocol ought to look something like this:
- “I hear you that you want to talk to X. That’s going to be very hard right now, because….”
- “But I don’t want to just take your name and contact information. I’ll do that too, of course. But they’ve asked me to try to do more than that, even though I’m only a receptionist/secretary/telephone operator. If you have some time to explain to me what’s going on and how you feel about it, I can promise to make sure that information gets to X, and to the rest of our management too. I’ll do that with your name or without your name, whichever you prefer.”
- Thereafter, listen. Ask occasional questions if you don’t understand. Make your questions open-ended, and make sure they don’t sound like an interrogation. For more on good question-asking, see the “Questioning” section of my “Empathy in Risk Communication” column.
- Resist the temptation to rebut, even if the person says something you know is false. Listen and take good notes. Ask questions to make sure that you got it, and to establish that you really are listening. Don’t comment, unless specifically asked. If the other person asks if you know the answer to some question, answer it if you can (and if you’re allowed). If the other person asks how you feel about something, give an honest, human answer (if you’re allowed). But this isn’t a dialogue; it’s the other person’s chance to vent, and your job is to listen empathically and keep a good record, not to vent back.

- While answering is inappropriate unless you’re asked, echoing can be helpful. See the “Listening and Echoing” section of “Empathy in Risk Communication” for some more advice on that. Especially when the call/visit is ending, or when you want to end it, try an echo: “Let me see if I understand your main points right. If I’m hearing you correctly, you’re angry about X, and you really want the company to do Y, and you’re worried that Z might happen. Would you say those are the three main things you want me to make sure our management hears?”

- Ask explicitly what sort of response the other person is looking for. Does s/he want a call back? A letter or email? Does s/he want to get onto a mailing list, or onto a committee? Did s/he just want to vent, and now that’s done? Don’t leave the impression that you have promised to accomplish whatever it is the other person wants to happen next, but make sure you have ascertained what that is.

- Say something about how little you have been able to help. “I realize you really wanted to be talking to X, not me.” “I understand that nothing the company can say is going to make you feel better about the fact that we did [whatever].” There’s reason to hope the other person will say that, actually, talking with you has been pretty helpful. (That’s the risk communication seesaw.) Even if s/he doesn’t, at least you will have established that you’re under no illusions of having solved the problem.
How do you engage people in mid-crisis long-term planning? Is it even possible?
| name: | Emily Jenke | |
| Field: | Community engagement and facilitation specialist | |
| Date: | June 15, 2009 | |
| Location: | Australia |
comment:
Whilst I never had the opportunity to meet you, you have done some significant work with my old organisation – the Department of Sustainability & Environment in Victoria. I worked for the Community Engagement Network in DSE for many years but happened to be on maternity leave when you worked with our team. Although I never experienced your knowledge first hand, your message has had a huge influence on the way I work!
I moved to South Australia two years ago and started my own business as a community engagement and facilitation specialist. Since then I have worked with the SA Government in health, natural resource management and fire preparedness.
I have been asked to offer my expertise (as a consultant) to the SA Government on the crisis unfolding in the Coorong, Lower Lakes and Murray Mouth (CLLMM). After years of unprecedented drought, the communities in the CLLMM region are facing an environmental catastrophe – acid sulphate soils being exposed due to extreme low water levels, long term salinity, no water available for households and stock, industry collapse, losing internationally recognised wetlands, the list goes on.
We have state and federal governments scrambling to react first to every piece of monitoring and trying to maintain the trust of an ever-sceptical community. It’s like Hurricane Katrina is happening over a 12-month period – the pace is excruciating, the effects are not visible from day to day, but this is a legacy that will be left for many generations to come. Not only are we seeing a slow environmental collapse, we are watching communities slowly die.
There are two ways the state government are approaching things at this time:
- Emergency response projects dealing with the current problems
- Seeking long-term sustainable solutions and learning from now
I am writing to you to seek your clarity on a major question that has me stumped!!!
For a long time I have been a true believer in the argument that you cannot “engage” a community that is in crisis. I believe it becomes a [one-way] communications exercise where messages must be given clearly and decisively. After having a surf around your website and many days of questioning myself, I am now doubting this belief.
In your words I sense we need an approach here that is includes precaution advocacy, crisis communication, and outrage management. It seems so complex to me, but is there a way in which we can “manage the crisis now” and also “plan the future” with the same people that are in the midst of this crisis. Do you believe that we can engage a community in driving the discussion forward while they are slowly “bleeding out”???
I’d be very interested in your thoughts and ideas – even if there is a paper somewhere on your website that might provide some clarity, that would be great. I suspect we are going to have to trail-blaze here in the way we engage, and there may not be an answer to our unique challenge, but I hoped it was worth a try!
Peter responds:
I am a firm believer in the possibility, efficacy, and wisdom of engaging with people in crisis situations. I don’t share the commonly expressed view that people in mid-crisis lose their sense of self-efficacy and autonomy and want “a strong leader” who takes charge, tells them what to do, and tells them what he (it is almost always a he) is going to do. People manage their fear/outrage better, obey official recommendations better, and find ways to help themselves better when they are part of the process of figuring out what to do and part of the implementation of whatever’s decided.
There’s some good evidence from the SARS outbreak in Singapore, for example, that people who felt the government was listening to their views on difficult decisions (whether to close the schools, whether to reveal the names of people under home quarantine, etc.) were less anxious, more compliant, and more confident of their own ability to cope.
The question you’re raising is a tougher one: whether people in crisis situations can be engaged vis-à-vis the long-term prognosis and a long-term strategy. For obvious reasons, people’s focus becomes very short-term in mid-crisis. It’s like Maslow’s hierarchy of needs: Getting through the crisis trumps planning the future.
On the other hand, there’s lots of reason to think that some mental picture of a possible future that’s achievable and acceptable can help people get through the crisis – it motivates resilience and protects against despair and denial. So while I probably wouldn’t ask people in mid-crisis to devote lots of time to detailed work on projects with only a long-term payoff, I would certainly engage them in visioning exercises about the long term: a collaborative effort to figure out where we’re trying to get to from the crisis situation we’re in, and a broad roadmap of how we might get there.
I don’t have any magic bullets, but here are a few off-the-cuff suggestions:
- I’d make use of the seesaw. Tell people you’re not sure they’re very interested in discussing the long term right now, in mid-crisis. Let them tell you you’re wrong, they really want to help develop a long-term vision for the region.
- Tell them how awful the current situation is. People like being told stories about themselves, and people in very difficult situations like the sense that others realize what they’re up against. Especially if you’re trying to engage them in long-term discussions, I think it will be essential to establish first that you know their short-term situation is bad. If they give you a seesaw response and tell you it’s not as bad as you’re saying, that’s okay too. But mostly you need them to know you know how bad it is.
- Tell them how little you can do to help – both with the short-term crisis and with the long-term problems. This is touchy. If you understate how much you can do, you’ll sound like you’re evading responsibility, and you’ll provoke outrage. If you overstate how much you can do, you’ll invite skepticism now (for overpromising) and much deeper outrage later (when you fail). The goal, I think, is to be explicit that you can do A and B and C to help with the short-term situation and D and E and F to help with the long-term situation – all the while insisting that that’s not much and apologizing for not being able to do more.

- Of course, don’t make A, B, C, D, E, and F a foreordained list. Ask them what they think you might be able to do. It’s always best, I think, to put some stuff on the table to start with (just A and D), but to let most of the action agenda (B, C, E, and F) evolve out of the engagement process. Some of what the group comes up with you may have had in mind anyway; some will be genuinely new.

- I think it’s critical to keep saying, sadly, that you can’t get people back to where they started. The old SA, the pre-drought, pre-climate change SA, is history. We can do a little to mitigate the changes that are coming; we can do a lot to adapt to those changes, and thus mitigate how devastating they are. What we can’t do is get back to where we were. If there are some silver linings – some ways in which the future looks preferable to the past – that’s fine; let them emerge. But I think it’s crucial in this kind of situation to keep saying that our goal is to make things “less worse” (than they would otherwise be) – making things better (than they were) is probably beyond us. Not everyone agrees with me that this is true, and not everybody who agrees it’s true agrees that it should be stressed. But I think people can’t really put their minds to problem mitigation until they get clear that they have to abandon the goal of getting things back the way they were.

- Despite the last few bullets, the focus shouldn’t be on what you can do for them. It should be on what they can do for themselves – short-term and long-term.

- You mention that you sense that public engagement in the situation you’re facing will require all three risk communication paradigms: crisis communication, precaution advocacy, and outrage management. I suspect you’re right. Crisis communication has a priority, in that the short-term crisis is at the top of everyone’s mind.

- But outrage management may also have a priority insofar as outrage at you (that is, at the SA government) may interfere with progress on anything substantive. This is an empirical question: Outrage (mostly fear) about the situation is helpful, but outrage (mostly anger) at the government for “mismanaging” it isn’t helpful, though it may (or may not) be justified. So if there’s a lot of outrage at the government, outrage management may have to precede or accompany crisis communication in order for the crisis communication to have any impact.

- Even precaution advocacy may have a priority. Incremental thinking that ignored long-term problems is a big piece of how we got into the mess we’re in, and insofar as people are still thinking short-term, you may need to frontload some long-term realism – which amounts to precaution advocacy vis-à-vis the long-term problems people want to ignore: (a) Here’s what the long-term future looks like if we don’t start addressing these problems now. It’s horrible. (b) Here’s what the long-term future might look like if we develop a plan and stick to it … which means more than just coping with the crisis we face right now. It’s not the way things used to be, and it may not be the way we wish things were, but it’s a whole lot better than the way things will turn out if we keep thinking short-term.
As I said, no magic bullets…. But I hope this helps a little.
Emily responds:
Thank you so much for sharing your “off the cuffs” with me – they do provoke reflection and also challenge the way I would have proceeded.
This is very much a community that is outraged – however, uniquely, they are outraged at governments from generations before! These state and federal governments made decisions 50–100 years ago (primarily around water over-allocation) which we bear the brunt of today. I think there are large parts of the community who are also angry and upset about the way the current and recent governments have approached “fixing” the problem, but there is mutual agreement across the board that what we are dealing with here in SA is very much the result of decisions made so long ago, by people who can no longer be held accountable. It’s a unique problem indeed.
I think with that perspective many of the people in the communities here can see the sense in moving forward and will be prepared to offer up their ideas and solutions. This does not negate the fact that those very same people will lose their livelihoods and the communities that they not only live in but have built to be what they are today. Our proximity (50 kms) to the State Capital of Adelaide intensifies the debate, as we have city people who “can’t water their gardens” adding complexity.
I find it fascinating that staff employed by governments at all levels believe they have to provide the answer – I clearly think their role is to ask the right questions of all players on the field, from scientists to townspeople and everything in between. Part of my role, I think, will be also challenging the way our government approaches this fragile issue, as well as provoking communities into action, or at least thinking about action! To me this feels like an opportunity to provide a “swift kick” to all involved and highlight the fact that while we have an unprecedented environmental catastrophe unfolding, likewise we need to approach it using “unprecedented” or “new” thinking.
I think our exchange provides another layer in the field of risk communication and engagement that we may see more of into the future, particularly in the context of the climate debate. We will see communities and nations bearing the brunt of decisions made generations before, and we need to start thinking about how we manage risk and engage people in positive ways with a slow, unfolding issue that may not be fully understood for decades.
Swine flu worst case scenarios: warn people now or wait till things start getting nasty?
| name: | Dan Rutz | |
| Field: | Government communications specialist | |
| Date: | May 30, 2009 | |
| Email: | dwr1@cdc.gov | |
| Location: | Georgia, U.S. |
comment:
Regarding your “Commentary” in Nature, and the longer version on your website:
As always I gained from your take on communication around A-H1N1. And as usual, I want to provoke you around an area about which you obviously feel strongly: the notion of speculating severe ill effect. I would challenge you on the need to do so, given what is known about this outbreak.
It is not because of fear over panic. I agree all the way with you that panic is rare, and I must have quoted you and Jody a dozen times during my Nepal-Bangladesh swing about your (and my) view that panic just doesn’t need to concern us. I remind government leaders that they apply the term “panic” to any behavior contrary to what they (the officials) want others to do.
I recall a tenet of risk communication is to err on the side of overreaction, but also to retain trust. Credibility, it would seem to me, requires us to come clean on what we know, and we have done that by stressing the uncertainties that surround this virus and the several outbreaks ascribed to it. Stressing the worse case scenario as I think you are suggesting would probably not result in people stocking up on peanut butter, but rather dismissing all or any concerns over the current outbreak. To take extreme action at this point simply doesn’t ring true to people, inasmuch as the disease remains mild in almost every instance. I would not be able to recommend ratcheting up the alarm at this point, for fear that it would be seen as “crying wolf” when there is none.
Let the uncertainty carry the day, I suggest. Allow us to suggest (by stressing what we don’t know) that people should be ready to act if this thing starts to turn nastier. We will know that – and that would be the time, I think, to get out the duct tape and pile on the staples.
And, too, I like to bear in mind that public health communication is often stress-provoking (by design, sometimes). Unnecessarily impairing the public’s quality of life “just in case” is a serious step. We need to bear in mind that our words have power, and we need to have a very good reason to upset people. When we must do so, I want people to know we’ve waited until we really needed to inconvenience them, and now that we have, we are hopeful they will have staked sufficient trust in us to follow our advice. Otherwise, it’s seen as overkill, and when the wolf really does arrive, the hens will be clucking away at their peril.
Thanks for letting me disagree, and for any thoughtful response you might send back.
I write as an individual, not for the CDC or the government.
Peter responds:
This is a tough question. And of course you’re right to raise it.
We agree that it’s crucial to stress uncertainty, including uncertainty about future severity. The question you’re raising is whether the worst case scenario and the advisability of preparing for it should be stressed. Consider two different statements:
Statement One: Flu is always unpredictable. We’re having enough trouble estimating the case attack rate and the case fatality rate of H1N1 so far. Since we’re no longer trying to test every case of influenza-like illness for H1N1, we don’t actually know how many cases there are. So we can’t calculate what percentage of those cases have died. And if we did have those numbers, we still wouldn’t have any reason to think the numbers are stable. H1N1 seems to be ebbing in the Northern Hemisphere as the weather turns warmer – but it’s too soon to tell for sure. What will it be like in the Southern Hemisphere, where the weather is getting colder? Will it return to the Northern Hemisphere after our summer? If it does, will it still be no more severe than a normal seasonal flu, or will it come roaring back in a much worse second wave? We have no answers to any of these questions.
Statement Two: H1N1 is pretty mild so far, compared to what we were – and still are – worried about. So far it’s a lot like having a second flu season – not a nonevent, but not a catastrophe either. We’re much less worried about the mild epidemic/pandemic we’re currently facing than about the possibility that it could get more severe. That’s what happened in 1918 – a mild first wave in the spring and then a severe second wave the following fall and winter. And there’s another possibility that has many experts very alarmed: the possibility that H1N1 could reassort with H5N1 to produce a new virus that is as transmissible as the former and as virulent as the latter. A severe pandemic could have untold consequences – not just the death and illness the pandemic itself would cause, but also the possible disruption of manufacturing and supply chains, which could lead to shortages of food, medicine, fuel, and other essentials. So we’re not out of the woods yet. We have no way of estimating the odds of H1N1 turning severe. It might – in which case preparing now could help ameliorate the disaster, even though no preparedness would be enough. It might not – in which case we would feel foolish for having prepared unnecessarily. That’s the dilemma: Do we prepare for the worst while we hope for the best, or do we simply hope for the best? On balance, we are doing the former, and we hope you will do the former as well. Here’s how.…
If I’m reading you right, you would be okay with the first statement but not the second. I want both.
I should point out that we’re talking about differences in degree, shades of gray. Even the first statement is more explicit about the uncertainties than most authorities have been most of the time. And even the second statement has all been said, albeit not as emphatically or frequently as I would like to see.
The two questions people ask in any emergency are: (a) what do you think is going to happen and (b) what’s the worst that could happen? The second question isn’t the literal worst case scenario; it’s the worst case that isn’t vanishingly unlikely, the worst case you’re actually worried about. These are the two questions we ask our doctor or our plumber: What do you expect and what are you worried about? In the case of H1N1, the answer to the first question is: We don’t know. Flu is unpredictable. The second question is the one you don’t want to answer.
I can see an argument for not stressing the worst case with publics that have no role in preparedness. And I can see an argument for not stressing cases so bad there’s no way to prepare. So I might deemphasize the second statement in developing countries, where preparedness for a severe pandemic of unknown probability isn’t a sensible prioritization of limited individual and societal resources. And even in developed countries, I might deemphasize what a pandemic with H1N1’s high CAR and H5N1’s astronomical CFR (61%) would be like. But governments in developed countries can prepare for a “severe” pandemic along the lines of 1918. And individuals in developed countries can do their share.
In fact, governments in developed countries are preparing for a 1918-like “severe” pandemic. The decision to produce an H1N1 vaccine, for example, is largely grounded in the fear that a second H1N1 wave might be severe enough to justify immunization, and the hope that if that’s the case a vaccine based on the current strain will be close enough to help. (The vaccine will also help protect people if and when this novel H1N1 becomes the newest seasonal flu virus.) What really infuriates me is to see governments taking the worst case seriously without saying that that’s what they’re doing, and without urging the rest of us to do likewise.
It’s not as if there were nothing for the rest of us to do. As you know, I think asking people to stockpile food, water, medications, and other supplies makes sense. The Bush administration urged people to do so back before H1N1 came on the scene, in preparation for a possible H5N1 or other pandemic. The risk of an H5N1 pandemic is no lower now than it was then. The risk of yet another novel flu virus arising is no lower now than it was then. We’ve simply added the risk of H1N1 turning more virulent to those other pandemic risks. How is it possible that storing cans of tuna under the bed made more sense without H1N1 than it makes with H1N1? If individual preparedness is unwise now, then it was also unwise when it was official HHS policy. I didn’t think so then, and neither did you.
Nor is “individual” preparedness all that’s at stake. We’re talking about all of civil society here – everything except government: churches, neighborhoods, companies, etc. The government’s failure to worry aloud about worst cases and encourage some preparedness for them is implicitly discouraging preparedness. Especially in a tough economy, people won’t make preparing a priority unless they are urged to do so and given coherent reasons to do so. That’s not happening.
So what’s the case against stressing the worst case and urging people to prepare for it? You address several possibilities.
The possibility that people might panic.
You join me in rejecting this one, so I won’t discuss it further.
The possibility that preparing is futile, that there’s nothing people can do.
I discussed this one above … and it’s not really one you raise (though others have raised it). You have done a lot of pre-pandemic risk communication work in places that many people argue have too few healthcare resources to “squander” any on pandemic preparedness. So I think you might be on my side of this one more emphatically than I am. Surely we agree that there are things middle-class individuals, companies, and community organizations can do to be better prepared (logistically and emotionally) for the “severe” 1918-like pandemic that might be coming.
The possibility that preparing is unnecessary, that there will be sufficient time to prepare after things get nasty.
This may turn out true. But I wouldn’t like to count on it. Especially as regards organizational preparedness for communities and companies, prepping takes time. And for individuals, the goal is to get as many people as possible already prepared before a severe pandemic looks imminent. Logistically, “rolling preparedness” means less stress on supply chains, less likelihood of shortages resulting from preparedness itself. Emotionally, it means more people who have already gotten through their adjustment reactions and are ready to roll – and ready to help others prepare.
How much warning time a flu pandemic will give us is one of many unanswerable questions. Before H1N1 arose, we thought a severe pandemic might appear very suddenly with very little warning time. Instead, we got a mild pandemic, and one that looks likely to back off the northern hemisphere for a few months. Arguably we’re getting more warning time than we thought we should count on. Do we now want to decline to use that warning time to prepare, in the expectation that we will have more warning time still to come?
The possibility that people might take our advice to heart, investing time, money, and anxiety in pandemic preparedness that could be better invested elsewhere.
This is simply so. As you rightly point out, preparing for a pandemic is a drain on people, materially and emotionally. We shouldn’t drain people pointlessly. But this seems to me to come back to #s 2 and 3. If preparing now is futile or unnecessary, then it’s unkind and unwise to drain people by asking them to prepare. But if preparing now is efficacious and useful, then we assess the benefit against the damage and decide whether the preparedness recommendation is justified.
Obviously, that’s a tough decision, given that we have no estimate of the probability of a future pandemic of varying degrees of magnitude. We can say pretty confident things, I think, about how much benefit to expect from preparedness; the benefit is greatest for a pandemic of intermediate seriousness – worse than 1957, 1968, and H1N1 so far; not as bad as H5N1-turned-transmissible. But without probability estimates, we’re stuck with this qualitative judgment: A pandemic worth preparing for seems (or doesn’t seem) likely enough to justify the burden of preparing for it. Most governments in developed countries have already decided that governmental preparedness makes sense. How can they reach this judgment and then decide that asking citizens to prepare as well is just too burdensome? That smacks of condescension.
The possibility that people might prepare, and then get angry if their preparedness turns out unnecessary.
You don’t raise this, but it could underlie some of #4. To some extent, I think, this is simply a price we decide to pay when we urge people to protect themselves against an uncertain risk. It’s the price weather forecasters pay when they call for an evacuation in the path of an oncoming hurricane (which might change directions or fizzle entirely). It’s the price we’re already paying for having warned people in the first few days of H1N1, when the early news from Mexico looked bad. In general, it’s a lower price than the price officials pay when they fail to warn people sufficiently about a risk that then materializes.
The price of recommending precautions that turn out unneeded can be ameliorated but not avoided entirely with good risk communication:
- Upfront acknowledgments in advance that “we’ll all feel foolish” if a severe pandemic never materializes.
- Candid confessions that “we don’t even know how likely one is.”
- Admissions that “so far our warnings have been wrong – SARS never went pandemic; neither did H5N1 (so far); H1N1 has been so mild (so far) that WHO doesn’t even want to use the word.
- Further acknowledgments, even apologies, if time passes and our warnings turn out in hindsight to have been excessive.
The possibility that people might ignore you – and you would lose credibility in the process.
This is your main concern, and it is far from a foolish concern. A mild H1N1 pandemic should have been a wonderful teachable moment – a chance to convince people that seasonal flu is a bigger deal than they imagined, and a chance to convince people that a severe pandemic is going to come sooner or later and preparing for it is simply the prudent thing to do. For a variety of reasons – not all of them avoidable – the teachable moment got frittered away. Instead, people are at risk of “learning” from H1N1 that even pandemics are no big deal and that public health authorities overreact to tiny threats in order to build their egos and their budgets.
If we stipulate that this is in fact what people have learned, then maybe it would only make things worse to try to warn them now that this mild pandemic could turn nasty, that it was a shot across our bow and has given us a chance to prepare properly for the severe pandemic that might be coming. Certainly it will take a lot of riskcomm skill to issue such a warning now. We will need a lot of empathy for those who respond with skepticism – and good-humored acceptance of the inescapable late-night jokes, “duct tape” redux.
I would be open to evidence from surveys or focus groups that the level of skepticism is currently so high that any efforts to describe worst case scenarios and urge preparedness will backfire.
Without evidence, my intuition is that things are not as bad as all that. I have talked to friends – one just yesterday – who are completely unconnected to the issue but have managed to piece together the reasons for concern about a more virulent second wave and for using the summer to prepare. This suggests to me that a wider segment of the public could learn the same lesson, if it were advanced more forcefully and more strategically.
I would love to work with CDC on ways to accomplish that objective.
Dan responds:
Dan’s response was organized point-by-point. In what follows, my original response is in the site’s regular serif type. Dan’s response-to-my-response is in sans-serif type on a blue background and boxed.
This is a tough question. And of course you’re right to raise it.
We agree that it’s crucial to stress uncertainty, including uncertainty about future severity. The question you’re raising is whether the worst case scenario and the advisability of preparing for it should be stressed. Consider two different statements:
Statement One: Flu is always unpredictable. We’re having enough trouble estimating the case attack rate and the case fatality rate of H1N1 so far. Since we’re no longer trying to test every case of influenza-like illness for H1N1, we don’t actually know how many cases there are. So we can’t calculate what percentage of those cases have died. And if we did have those numbers, we still wouldn’t have any reason to think the numbers are stable. H1N1 seems to be ebbing in the Northern Hemisphere as the weather turns warmer – but it’s too soon to tell for sure. What will it be like in the Southern Hemisphere, where the weather is getting colder? Will it return to the Northern Hemisphere after our summer? If it does, will it still be no more severe than a normal seasonal flu, or will it come roaring back in a much worse second wave? We have no answers to any of these questions.
Statement Two: H1N1 is pretty mild so far, compared to what we were – and still are – worried about. So far it’s a lot like having a second flu season – not a nonevent, but not a catastrophe either. We’re much less worried about the mild epidemic/pandemic we’re currently facing than about the possibility that it could get more severe. That’s what happened in 1918 – a mild first wave in the spring and then a severe second wave the following fall and winter. And there’s another possibility that has many experts very alarmed: the possibility that H1N1 could reassort with H5N1 to produce a new virus that is as transmissible as the former and as virulent as the latter. A severe pandemic could have untold consequences – not just the death and illness the pandemic itself would cause, but also the possible disruption of manufacturing and supply chains, which could lead to shortages of food, medicine, fuel, and other essentials. So we’re not out of the woods yet. We have no way of estimating the odds of H1N1 turning severe. It might – in which case preparing now could help ameliorate the disaster, even though no preparedness would be enough. It might not – in which case we would feel foolish for having prepared unnecessarily. That’s the dilemma: Do we prepare for the worst while we hope for the best, or do we simply hope for the best? On balance, we are doing the former, and we hope you will do the former as well. Here’s how….
If I’m reading you right, you would be okay with the first statement but not the second. I want both.
Dan: I’m actually okay with both statements, as they amplify the uncertainties flu planners (we) are facing, as well as present the dilemma openly: Given the uncertainties, what is the prudent course? I present these very issues in my workshops as well, including the possibility of an A-H1N1 / H5N1 recombination. The argument is, I think, best used in defending the emphasis WHO and HHS/CDC have placed on preparedness around this new threat: why vaccine development is critically important even though it is costly and logistically challenging (e.g. the likelihood that people will need two or three flu shots next fall instead of one).
Then there’s the nagging issue of vaccine safety. Perhaps you’ll recall that the last time we offered a swine flu vaccine (1976–77; I was a young TV reporter in Madison at the time, quite out of the CDC loop), the vaccine caused a high rate of Guillain-Barré syndrome – which I’ve recently learned may have been caused by an antibody reaction unique to vaccine formulations targeting swine-originated viruses. That possibility raises safety questions I’m sure will need to be addressed when the pilot vaccine is ready for testing. I’m anticipating a need to be forthright about vaccine uncertainties, assuming (as I shall) that those safety tests will not settle the issue once and for all.
I should point out that we’re talking about differences in degree, shades of gray. Even the first statement is more explicit about the uncertainties than most authorities have been most of the time. And even the second statement has all been said, albeit not as emphatically or frequently as I would like to see.
The two questions people ask in any emergency are: (a) what do you think is going to happen and (b) what’s the worst that could happen? The second question isn’t the literal worst case scenario; it’s the worst case that isn’t vanishingly unlikely, the worst case you’re actually worried about. These are the two questions we ask our doctor or our plumber: What do you expect and what are you worried about? In the case of H1N1, the answer to the first question is: We don’t know. Flu is unpredictable. The second question is the one you don’t want to answer.
Dan: Continuing the narrative from above, there are a ton of uncertainties we can and must address at this point, and the “worst case” scenario ought to be part of that discussion. What I’m less sure of is how much of that worry need/should we load on the shoulders of a largely unconcerned (and presently unthreatened) lay public. Just what do we expect them to do?
I can see an argument for not stressing the worst case with publics that have no role in preparedness. And I can see an argument for not stressing cases so bad there’s no way to prepare. So I might deemphasize the second statement in developing countries, where preparedness for a severe pandemic of unknown probability isn’t a sensible prioritization of limited individual and societal resources. And even in developed countries, I might deemphasize what a pandemic with H1N1’s high CAR and H5N1’s astronomical CFR (61%) would be like. But governments in developed countries can prepare for a “severe” pandemic along the lines of 1918. And individuals in developed countries can do their share.
Dan: I’d give a break to publics in both developed and developing countries. I want our publics to be supportive of government planning; I want private concerns to dust off their pandemic preparedness plans and get their “just-in-case” adjustments ready to go. And we have (through ECS teams) had a number of calls with business and industrial leaders to remind them of that. I’m not sure a focus on the worst case will help much, though, with the man/woman on the street. They’re just not about to start stockpiling food and I think we’d be widely mocked for suggesting it at this stage of the game.
In fact, governments in developed countries are preparing for a 1918-like “severe” pandemic. The decision to produce an H1N1 vaccine, for example, is largely grounded in the fear that a second H1N1 wave might be severe enough to justify immunization, and the hope that if that’s the case a vaccine based on the current strain will be close enough to help. (The vaccine will also help protect people if and when this novel H1N1 becomes the newest seasonal flu virus.) What really infuriates me is to see governments taking the worst case seriously without saying that that’s what they’re doing, and without urging the rest of us to do likewise.
Dan: Consider the complexities of life in the 21st century. I think even well-fed and advantage-laden Americans have a pretty extensive worry agenda. I like to see our job as assuming a major part of that concern, until we get closer to a point where we really DO need to move people to personal action. We’ve been there in some areas; e.g., Mexico City, New York, Milwaukee, where local outbreaks appropriately triggered social distancing mandates, at great political risk, economic/social disruption, and inconvenience. Those moves were brave and justified. But I’d hold we don’t all have to start biting our nails in fear of what might happen six months from now. Peter, life’s just too damn short. Yeah, I want the flight attendant to remind me of where the exits are and how to don the lifejacket, but I don’t need to see a video of a plane crashing in flames, even though that’s the worst case scenario every time I board.
It’s not as if there were nothing for the rest of us to do. As you know, I think asking people to stockpile food, water, medications, and other supplies makes sense. The Bush administration urged people to do so back before H1N1 came on the scene, in preparation for a possible H5N1 or other pandemic. The risk of an H5N1 pandemic is no lower now than it was then. The risk of yet another novel flu virus arising is no lower now than it was then. We’ve simply added the risk of H1N1 turning more virulent to those other pandemic risks. How is it possible that storing cans of tuna under the bed made more sense without H1N1 than it makes with H1N1? If individual preparedness is unwise now, then it was also unwise when it was official HHS policy. I didn’t think so then, and neither did you.
Dan: Medication stockpiling is controversial; there’s not enough Tamiflu if everyone did it. Transparency, I suppose, requires us to admit the conflict of interest we have in public health of wanting, on the one hand, to assure order in the clinical setting, but thinking (I agree with you on this) that it makes sense to have your own medicine stash.
Could we compromise here? Give people permission to stockpile food, etc., but don’t push it on everyone; that way, we’re respecting those who choose to be cautious, but not antagonizing those who decide to wait it out a bit longer.
Nor is “individual” preparedness all that’s at stake. We’re talking about all of civil society here – everything except government: churches, neighborhoods, companies, etc. The government’s failure to worry aloud about worst cases and encourage some preparedness for them is implicitly discouraging preparedness. Especially in a tough economy, people won’t make preparing a priority unless they are urged to do so and given coherent reasons to do so. That’s not happening.
So what’s the case against stressing the worst case and urging people to prepare for it? You address several possibilities.
The possibility that people might panic.
You join me in rejecting this one, so I won’t discuss it further.
The possibility that preparing is futile, that there’s nothing people can do.
I discussed this one above … and it’s not really one you raise (though others have raised it). You have done a lot of pre-pandemic risk communication work in places that many people argue have too few healthcare resources to “squander” any on pandemic preparedness. So I think you might be on my side of this one more emphatically than I am. Surely we agree that there are things middle-class individuals, companies, and community organizations can do to be better prepared (logistically and emotionally) for the “severe” 1918-like pandemic that might be coming.
The possibility that preparing is unnecessary, that there will be sufficient time to prepare after things get nasty.
This may turn out true. But I wouldn’t like to count on it. Especially as regards organizational preparedness for communities and companies, prepping takes time. And for individuals, the goal is to get as many people as possible already prepared before a severe pandemic looks imminent. Logistically, “rolling preparedness” means less stress on supply chains, less likelihood of shortages resulting from preparedness itself. Emotionally, it means more people who have already gotten through their adjustment reactions and are ready to roll – and ready to help others prepare.
How much warning time a flu pandemic will give us is one of many unanswerable questions. Before H1N1 arose, we thought a severe pandemic might appear very suddenly with very little warning time. Instead, we got a mild pandemic, and one that looks likely to back off the northern hemisphere for a few months. Arguably we’re getting more warning time than we thought we should count on. Do we now want to decline to use that warning time to prepare, in the expectation that we will have more warning time still to come?
Dan: This is where human nature runs against risk communication idealism. Even in the hard-hit areas, I would expect memories will be short and the extent of preparedness you espouse just isn’t going to happen. “We got through it; the schools reopened; it wasn’t all that bad.” I’m afraid too much focus on the PUSH for active engagement will only boost denial rather than the adjustment reaction. The latter doesn’t kick in until people feel and accept the threat. Just talking about it (especially, perhaps, the government – which people tend not to take all that seriously in the first place) isn’t going to make people wake up and say, “Oh my God, CDC says this could be real bad. I’m going to drop everything and head to the Wal-Mart for canned goods.” (Remember Leavitt’s tuna-under-the-bed suggestion; Leno had a field day.)
The possibility that people might take our advice to heart, investing time, money, and anxiety in pandemic preparedness that could be better invested elsewhere.
This is simply so. As you rightly point out, preparing for a pandemic is a drain on people, materially and emotionally. We shouldn’t drain people pointlessly. But this seems to me to come back to #s 2 and 3. If preparing now is futile or unnecessary, then it’s unkind and unwise to drain people by asking them to prepare. But if preparing now is efficacious and useful, then we assess the benefit against the damage and decide whether the preparedness recommendation is justified.
Obviously, that’s a tough decision, given that we have no estimate of the probability of a future pandemic of varying degrees of magnitude. We can say pretty confident things, I think, about how much benefit to expect from preparedness; the benefit is greatest for a pandemic of intermediate seriousness – worse than 1957, 1968, and H1N1 so far; not as bad as H5N1-turned-transmissible. But without probability estimates, we’re stuck with this qualitative judgment: A pandemic worth preparing for seems (or doesn’t seem) likely enough to justify the burden of preparing for it. Most governments in developed countries have already decided that governmental preparedness makes sense. How can they reach this judgment and then decide that asking citizens to prepare as well is just too burdensome? That smacks of condescension.
Dan: Not condescension, to my mind, but compassion. We’re doing what we can to prepare; we’re offering you the chance to do the same, but we’d like to spare you the ordeal of shouldering the worst case scenario until such time as we have reason to believe you really need to. We’re just too far out to make that call, but stay tuned.
Floridians should know how to protect their homes from hurricanes, but we’re not suggesting now that everyone start covering the windows with plywood. We WILL ask them to do that when the storms take shape and start drifting eastward.
The possibility that people might prepare, and then get angry if their preparedness turns out unnecessary.
You don’t raise this, but it could underlie some of #4. To some extent, I think, this is simply a price we decide to pay when we urge people to protect themselves against an uncertain risk. It’s the price weather forecasters pay when they call for an evacuation in the path of an oncoming hurricane (which might change directions or fizzle entirely). It’s the price we’re already paying for having warned people in the first few days of H1N1, when the early news from Mexico looked bad. In general, it’s a lower price than the price officials pay when they fail to warn people sufficiently about a risk that then materializes.
The price of recommending precautions that turn out unneeded can be ameliorated but not avoided entirely with good risk communication:
- Upfront acknowledgments in advance that “we’ll all feel foolish” if a severe pandemic never materializes.
- Candid confessions that “we don’t even know how likely one is.”
- Admissions that “so far our warnings have been wrong – SARS never went pandemic; neither did H5N1 (so far); H1N1 has been so mild (so far) that WHO doesn’t even want to use the word.
- Further acknowledgments, even apologies, if time passes and our warnings turn out in hindsight to have been excessive.
Dan: Not angry, but dismissive. If we run people up and down the fear scale too soon, too often, they may not get mad, but instead annoyed and dismissive. They just won’t pay attention when we’re surer of the impending threat.
The possibility that people might ignore you – and you would lose credibility in the process.
This is your main concern, and it is far from a foolish concern. A mild H1N1 pandemic should have been a wonderful teachable moment – a chance to convince people that seasonal flu is a bigger deal than they imagined, and a chance to convince people that a severe pandemic is going to come sooner or later and preparing for it is simply the prudent thing to do. For a variety of reasons – not all of them avoidable – the teachable moment got frittered away. Instead, people are at risk of “learning” from H1N1 that even pandemics are no big deal and that public health authorities overreact to tiny threats in order to build their egos and their budgets.
If we stipulate that this is in fact what people have learned, then maybe it would only make things worse to try to warn them now that this mild pandemic could turn nasty, that it was a shot across our bow and has given us a chance to prepare properly for the severe pandemic that might be coming. Certainly it will take a lot of riskcomm skill to issue such a warning now. We will need a lot of empathy for those who respond with skepticism – and good-humored acceptance of the inescapable late-night jokes, “duct tape” redux.
I would be open to evidence from surveys or focus groups that the level of skepticism is currently so high that any efforts to describe worst case scenarios and urge preparedness will backfire.
Without evidence, my intuition is that things are not as bad as all that. I have talked to friends – one just yesterday – who are completely unconnected to the issue but have managed to piece together the reasons for concern about a more virulent second wave and for using the summer to prepare. This suggests to me that a wider segment of the public could learn the same lesson, if it were advanced more forcefully and more strategically.
I would love to work with CDC on ways to accomplish that objective.
Dan: As you say, #6 is my major concern. That’s why I fall back on “sharing the dilemma” with reporters and others who can reach or influence the masses. In public health we’re always confronted by planning for the emergency that doesn’t come (and being accused of overreacting) vs. downplaying the threat that does (and not warning people in time). I want reporters, especially, to be reminded of this ever-present quandary. Having said that, and reflecting on this discussion, I think you’d see my main flaw here as being overly practical. As much as I want people to agree with me and you on taking the threat seriously, I’m pretty sure that nothing I or the government can say is going to budge the needle in that direction. There’s just too much else going on in life for this issue to emerge as one requiring a lot of time, money, and worry. The best we might hope for is to very loudly defend our actions, based on worse case scenario concerns, and be ready to sound the alarm when we might more reasonably expect people to actually do something.
WHO’s “Outbreak Communication Guidelines” – and calling a pandemic a pandemic
| name: | Liz Smith | |
| Field: | Environmental communication | |
| Date: | May 26, 2009 | |
| Location: | Georgia, U.S. |
comment:
Interested readers also may wish to take a look at the WHO manual on Outbreak Communication: Best Practices for Communicating with the Public during an Outbreak. ![]()
Peter responds:
As the world copes or prepares to cope with swine flu H1N1, now is a good time to call risk communicators’ attention to the World Health Organization’s guidelines for communicating with the public during an infectious disease outbreak.
There are six documents of interest.
- “ WHO Outbreak Communication Guidelines” – This eight-page document, published by WHO in 2005, is based largely on an “Expert Consultation on Outbreak Communications” conference held in Singapore in September 2004. It has sections on “Trust,” “Announcing Early,” “Transparency,” “The Public,” and “Planning.”
- Outbreak Communication: Best Practices for Communicating with the Public during an Outbreak – This is the 59-page report of the Singapore “Expert Consultation on Outbreak Communications” conference. It puts meat on the bones of the “WHO Outbreak Communication Guidelines.”
- “World Health Organization Outbreak Communication Planning Guide (2008 edition)” – This 30-page manual outlines a process “to help national authorities apply the WHO Outbreak Communication Principles to their outbreak planning and preparation activities.”
- “Outbreak Communication – The Goal, Strategies and Controversies: Evidence and Experience” – This 24-page draft “background document” was written in preparation for the Singapore conference. It includes a five-page discussion of trust, accountability, and transparency. Many recommendations from that section made it into the “Guidelines.” The recommendation to “Acknowledge and apologize for errors” did not.
- “Outbreak Communications Guidelines: Appendices” – This 21-page document consists of nine appendices to the pre-conference draft “background document,” including “Not Informing the Public Early,” “Limited Findings about False Alarms,” and “Examples of Outbreak Strategies.”
- “Outbreak Communications Guidelines: Evaluating and Coaching” – This 12-page supplement to the pre-conference draft “background document” focuses on recommendations for ways to evaluate outbreak communication efforts quickly and cheaply.
I attended the Singapore conference and played a role in drafting the “Outbreak Communication Guidelines” and its attendant reports and manuals, etc. My wife and colleague Jody Lanard played a much bigger role, and is credited with writing the last two of the six documents listed above.
The “Outbreak Communication Guidelines” are aspirational. That is, it is easy to find examples where governments (and WHO itself) have fallen short of the principles articulated in these six documents. Nonetheless, I think they have had a real impact. Their greatest value, I suspect, is as ammunition for internal battles among government risk communicators. When there’s a debate over whether to be candid about X or whether to involve the public in Y, those arguing in the affirmative can point out that “WHO says we should.”
The WHO “Guidelines” and the definition of a pandemic
Jody drafted the rest of this response.
The “Outbreak Communication Guidelines” themselves describe some crucial concepts which some national leaders accept only in principle. This was evident last week at the World Health Assembly, when health ministers from many countries pleaded with WHO not to raise the pandemic phase to Phase 6, although current conditions seemed to match the definition of Phase 6, or at the very least, the definitions that were in place ![]() from 1999 until April 26, 2009.
from 1999 until April 26, 2009.
Under the heading “Trust,” the first of five “best practices,” the “Guidelines” state:
Trust in communicating with the public is critical in both directions. Evidence shows that public panic is rare and most rare when people have been candidly informed. But the extent to which outbreak managers trust the public’s ability to tolerate incomplete and sometimes alarming information influences communication decision-making and effectiveness.
When WHO deferred to the urgent pleading of member states to keep the pandemic phase at 5, there was clear evidence that those doing the pleading do not trust their publics to handle alarming news. They believe that their publics will grossly overreact.
The “Guidelines” also recommend being responsive to the public. And WHO member states are certainly one of WHO’s publics. Under the fourth heading, “The public,” is the recommendation that “the public’s concerns must be appreciated.… When a publicly held view has validity, policy-making should be consistent with that view.”
And the “Best Practices” report elaborates on trust between organizations:
Trust is also essential between different organizations. The importance of having common assessments among partners in the midst of an outbreak was stressed by some participants.…
So it is appropriately responsive to take the member countries’ strongly-held views into consideration. Their deeply-felt perception that they would not be able to lead their citizens successfully through the initial shock of learning that swine flu is causing a pandemic deserved respect. However much I may disagree with leaders’ views of their citizens’ fragility, it is responsive of WHO to take those opinions into account. This is not the point at which WHO failed to honor its own guidelines.
The point of failure comes under the third heading, “Transparency,” where the “Guidelines” state that communication should be “candid, easily understood, complete and factually accurate,” and that “Total candour should be the operational goal.…”
Discussing barriers to transparency, the “Guidelines” state:
Economic arguments are often raised, but public health officials’ first concern has to be human health. There is, however, an increasing body of evidence showing that recovery from the economic impact of an outbreak is faster when governments have been transparent and have developed a track record of effective outbreak management.
In the course of agreeing to reconsider its definition of a pandemic, “transparency” means, at the very least, that WHO should have acknowledged to the public-at-large the “factually accurate” reality that according to its 1999 pandemic phase definition, and according to its 2005 pandemic phase definition, and quite likely according to its long-considered but abruptly substituted April 26 2009 pandemic phase definition, the current situation qualifies as a pandemic, albeit at this time an apparently mild pandemic.
With that acknowledgement, WHO could have lived up to its own outbreak communication standards – being transparent; appreciating the concerns of its various publics; and working to build, maintain, or restore trust.
It isn’t necessarily too late. This would be a good time for WHO to reconsider adding “Acknowledge and apologize for errors” under the “Trust” or “Transparency” section of the “Guidelines.”
Managing the outrage of extremists
| name: | Rusty Cawley | |
| Field: | Public relations | |
| Date: | May 18, 2009 | |
| Email: | rcawley@tamu.edu | |
| Location: | Texas, U.S. |
comment:
Almost everything we discuss in outrage management deals with publics that are both tangible (in that you generally know where to find them and thus can communicate with them) and manageable (within limits).
But what about outraged publics that are neither tangible nor manageable?
For example, animal rights extremists. Here is a public that is so outraged by animal research that its members have established a virtually invisible network to strike back at institutions and scientists with violence (real and implied). When these folks target a client company or individual, are there ways to mitigate their outrage and thus help protect the client? (Let’s assume that the client is meeting all federal and professional standards for the ethical treatment of research animals, is engaging in legitimately useful research, and is unwilling to simply abandon animal-based research.)
Is this task within the scope of outrage management?
Peter responds:
Since you mention violence, I need to start there. Whatever it is that makes people turn violent, outrage is surely part of the mix, so in principle outrage management might help deter a violent opponent. But only in principle. Far more than outrage is going on, and the outrage itself is too high, too unreachable, and certainly too dangerous to try to manage. The appropriate response to violence or the threat of violence, I believe, is to call the cops – not the communication consultants.
That said, I should immediately add this important qualifier. You mention “implied” violence, and that makes me a bit leery. Rudeness isn’t violence. Vaguely hostile muttering isn’t violence. Even lawbreaking isn’t necessarily violence. It’s often a mistake to call the cops simply because protesters are trespassing and shouting profanities. There may be better ways – outrage management ways – to defuse the situation.
But if you fear for your safety, or even the safety of your property, call the cops.
Even more than “violence,” “extremism” is largely in the mind of the beholder. We need to be careful whom we label as extremists, even to ourselves. (It’s worth noting that groups and individuals may call themselves “radical,” but rarely “extremist”; the word is intrinsically pejorative.) I have certainly had clients who described as “extremist” people and groups that didn’t seem all that extremist to me. And government agencies and corporations have sometimes labeled me as “extremist” with regard to my calls for radical candor and transparency.
If we’re talking about extreme means, then maybe violence or something close to violence is part of the “extremist” package. Extreme beliefs are a different story. Jainism, for example, is pretty extreme on the subject of animal rights, believing that all living creatures have souls. But it’s very hard to imagine a violent Jain animal rights activist.
I don’t know if you would consider a nonviolent animal rights activist (Jain or otherwise) an extremist or not. But let’s assume that the problem is how to deal with extremist ideology, not extremist tactics – how to deal with nonviolent opponents whose opinions are very far from the mainstream, even the mainstream of other opponents.
That leaves open whether or not those with extremist views are outraged (upset, angry, frightened, etc.). They may be icy calm. They may be calm but feigning outrage, for the sake of greater appeal to the media and the stakeholders they are hoping to woo to the cause. Or they may be genuinely outraged themselves.
Assuming you think they’re outraged, is it useful to try to reduce their outrage? I think the answer is yes. Whether they’re extremists or not, outraged people are rarely willing to compromise. Of course even a calm extremist may decide, for strategic or ideological reasons, to stay pure rather than bargain. But an outraged extremist will automatically refuse to bargain. So if negotiation is your goal, outrage management is worth a shot.
Playing to the “attentives”
Despite all of the above, most interactions with (ideological) extremists should be viewed as theater. Odds are, your goals and theirs are incompatible. What you might consider an acceptable compromise is probably totally unacceptable to them; what they might consider an acceptable compromise is probably totally unacceptable to you. (Does that make you an extremist in their eyes?) Whether they’re calm or outraged – and whether you’re calm or outraged – there probably isn’t going to be a meeting of the minds.
What’s left, then, is how your interaction with your extremist opponents affects other stakeholders. In my column on “Stakeholders,” I draw the distinction between “fanatics” and “attentives.” (Note that the word “fanatic” is almost as offensive as “extremist” in some circles. It should be used sparingly.) The fanatics are deep, strong opponents; the attentives may tend to oppose you too, but less obsessively and less unalterably. The column continues:
How do you end the controversy? The best way is to get the fanatics to declare victory, under conditions you can live with. Satisfying your most fanatic stakeholders isn’t always feasible, but if it’s feasible it is always advisable. Second best is to persuade the attentives that the fanatics have won enough. They may still not be satisfied (fanatics are like that), but now you’re quarreling over table scraps, and the attentives are getting bored. A distant third is to persuade the attentives that the fanatics are wrong; this is soul-satisfying when it happens, but it is usually a great deal harder than the first two options.
Option 2 is the one you should aim for, I think, when dealing with people and groups you consider extremist. Trying to win them over is a waste of time, and even trying to negotiate a mutually acceptable compromise is a long shot. Trying to persuade the attentives that you’re right and the extremists are wrong (and extremists!) is also very difficult. In fact, it can easily backfire. Your best course is to convince the attentives that you respect the extremists and their views, that they have already successfully forced you to make some important concessions, and that it’s time to move on.
Let me spell this out in the form of four guidelines. These are not guidelines for managing the outrage of extremists. Rather, they are guidelines for talking about extremists in a way that manages the outrage and potential outrage of attentives:
- Document how extremists have forced you to improve. This is the single most important guideline. Most people – even most attentives – don’t want the extremists to succeed totally; their goals are too extreme. But people don’t want you to succeed totally either. They want the extremists to win some early battles, and then lose the war. So to the extent that you can do so honestly, depict your improvements as (partial) responses to pressure from the extremists, not as examples of your inherent goodness (and proof that the world doesn’t need extremists).
- Tolerate some immoderate conduct from extremists. There is a “seesaw” operating here. If you overreact to rudeness (for example) on the part of extremists, others at the meeting may well rally to their cause. If you’re long-suffering and tolerant, on the other hand, others are a lot likelier to resent the extremists’ conduct. Ideally, you will wind up defending the extremists’ right to disrupt the meeting, while the attentives roll their eyes and wish you’d run a tighter ship. A side benefit: Those who might be tempted to be a little disruptive themselves tend to think again when they see how people are reacting to the extremists: “I’m not like them.”
- Distinguish the extremists’ views from their behavior. If extremists are acting in ways you can’t tolerate, be explicit about the distinction between their views and their actions. I have had a number of timber industry clients over the years that were victims of activist vandalism. In each case, I urged the company to remind the activists – publicly – how many legal avenues were available. “They have a position that deserves to be heard, and there are many ways for them to make sure they are heard, from news conferences to lawsuits to legal demonstrations. Vandalism is not the American way. We hope they will come to next Tuesday’s meeting and express their views freely.”
- Describe extremists’ extremist ideology accurately and respectfully. Almost by definition, the views of attentives are a lot more moderate than the views of extremists. It is useful to make sure attentives are aware of the discrepancy. But you have to do so respectfully. It’s almost never wise to attack extremist ideology as extremist. Instead, describe that ideology so accurately and so respectfully that the extremists can find nothing to take offense at … while the attentives start to rethink the company they’re keeping.
You mention that extremist groups may be “invisible” rather than “tangible,” especially if their members are doing illegal things. Obviously, that makes it close-to-impossible to manage the extremists’ outrage. But if anything, it makes it easier to manage the attentives’ outrage. You can give the extremists credit for your improvements, express tolerance for their rudeness or other misconduct, distinguish their views from their behavior, and describe their extremism respectfully … all without any extremists actually present in the room.
I want to reiterate that I’m talking about extremist views here, not extremist actions. I would not urge a client to express tolerance for violence, or to give credit to violent acts as the impetus for positive change. As you put it, violence is outside “the scope of outrage management.” Extreme views, on the other hand, are well within the scope of outrage management – but the outrage to be managed is usually the outrage of attentives, not of the extremists themselves.
Two animal rights stories
Since you mention animal rights controversies, let me end with two animal rights examples of the fourth guideline – one short one and one long one.
A few years ago, an environmental group client successfully advocated new regulations that required far more animal testing of potentially hazardous chemicals. People for the Ethical Treatment of Animals came out against the new regs. In addition to suggesting some programmatic changes they could credit to PETA and its allies (guideline #1), my client also went out of its way to say things like this: “Those who believe that animals ought to have the same rights as human beings are necessarily opposed to animal testing no matter how many human lives it could save. This is a coherent philosophical position that we respect but do not share.” Most of PETA’s contributors don’t share it either, of course. This kind of respectful labeling can help remind attentives that the extremists have won a lot already, and that they don’t actually want the extremists to win it all.
Many years earlier, animal rights activists had organized against a cosmetics company client, accusing it (accurately) of killing and tormenting large numbers of rabbits in order to test various product ingredients. Eventually, my client approached its leading opponent with the following offer:
You believe that our testing program kills rabbits unnecessarily, and you think it’s morally wrong. We think the program is necessary. But you have taught us that killing animals does raise moral problems, even when it’s necessary. You think it’s an unnecessary evil. We think it’s a necessary evil. But we agree that it is evil. So we want to establish a Fund for Rabbits. We will pay into that fund a specified amount for every rabbit that dies as a result of our testing program – enough to support other endangered rabbits in a high-quality lifestyle. We want to make sure we can honestly say that more rabbits are alive, and happy, as a result of our testing program than would be the case if the program were ended. And we want you to administer our Fund for Rabbits.
Put yourself in the position of the animal rights group. If you agree to run the fund, you will greatly offend your core activists, who will see you as selling out. If you refuse to run the fund, you will greatly confuse your casual members, who won’t understand why you turned down a chance to save and nurture beautiful bunnies. You’re either going to look too moderate to your extremist volunteers or too extremist to your moderate contributors. You can’t win.
So the group came back to my client and asked, “What will you do if we accept?” “Publicize your acceptance,” my client responded. “And what will you do if we refuse?” “Publicize your refusal.” Long pause. “What would it take for you not to go public?” “Leave us alone.” For some years thereafter, that particular animal rights organization refrained from attacking that particular cosmetics company.
Note: Rusty Cawley has written an extended response, which is posted on this site. In it he distinguishes animal rights extremists from animal rights activists, and outlines the way he thinks a university research laboratory (such as the one he works for) should deal with each.
Selling pandemic prep to family and friends
| name: | Elenor Snow | |
| Field: | Peter’s webmaster | |
| Date: | May 18, 2009 | |
| Location: | Georgia, U.S. |
comment:
I’m working to … sufficiently alarm … family and friends to try to get them to prepare for a possible pandemic. I have to keep it short, because they won’t bother with a long, reasoned discussion of the details; I’m trying to just get their attention and get them to at least do the minimum, including begin to pay closer attention (you know, move them from “inattentives” to “attentives”).
This is my message to them. Comments? Help? Focus-change?
Family and friends:
Please start paying attention to this. The government and media are still not telling people to prepare to “shelter in place” (as they call it for terrorism): to lay in food and water and prescription meds in the event it DOES become that second deadly wave and you daren’t go out! Please stock up on food, meds, water, gas, cash, pet food, and anything else you might need for, say, a two-week lockdown. (If you can afford it and your doc will go along, try to get a Tamiflu and/or Relenza prescription – and try to find a pharmacy that has some! Lots of them are now out.)
No one “official” (well, except maybe Joe Biden) is preparing. Our “just-in-time” supermarkets are still laying in supplies to sell now – but if it does turn out to be the big one, you won’t be able to buy supplies then!
Our medical professionals don’t seem nearly educated enough in preparation (and maybe even treatment!) since they’re so busy pooh-poohing people’s reasonable requests for Tamiflu prescriptions as “panic.”
If this were a category-5 hurricane approaching, the government would be telling people to board up their windows and lay in food and water, whether or not they knew if it would land or veer out to sea (or fizzle to a cat-1 before landing – pray God this possible pandemic fizzles!!). That’s the whole point of preparing! The government has sent out to the states one-fourth of the national stockpile of Tamiflu and Relenza, but the states don’t seem to have in place good solid plans for how they’re going to USE the drugs – like who gets them, when, and how.
The WHO pandemic phases are (in my amateur view) sort-of the equivalent of the tornado preparations system. A tornado WATCH means “keep an eye out, prepare to go to shelter.” A tornado WARNING means “go to your basement NOW – do not wait until you can see and hear the darned thing up your street!”
In a tornado watch, you batten down your hatches and make sure you’re ready to ride it out if it comes.
We’re in – or should be in – “pandemic flu watch” – preparing in case we have to duck, boarding up our metaphorical windows in case it lands in our neighborhood. The government will probably declare the “flu-hurricane warning” too late – and if you had not prepared yourself and your family during “flu watch,” there won’t BE any supplies for you to prepare with as this flu-hurricane lands in your neighborhood.
And, oh please, this is NOT NOT NOT panic! Do you consider keeping antibiotic salve in your medicine chest to be “scrape panic”? Or having a fire extinguisher in your kitchen “fire panic”? Preparing for what MAY be a “flu-hurricane” is not panic. It is reasonable, rational preparations for an emergency that may or may not arrive! You can’t prepare for an emergency AFTER it arrives!
Peter, help me wake up my loved ones!
Peter responds:
I have only one quarrel with the content of what you’re saying: I do think officials are preparing, at least for a comparatively mild pandemic like those in 1957 and 1968. But I think you’re right that they’re not very aggressively urging the rest of us to prepare too – and they’re certainly not urging preparedness for something more severe, like the pandemic of 1918. So, like you, I have been trying to do the job for them, harassing family and friends to get ready for the possibility of a pandemic severe enough to disrupt our lives.
I try to remember to harass them gently – or, as you would put it: GENTLY!
Bear in mind that the people we’re talking to aren’t hearing about the risk of a swine flu pandemic for the first time. They’ve heard a good bit about it already over the past few weeks, and what they’ve heard hasn’t persuaded them to prepare as much as you and I think they should. People are not blank slates, waiting for us to write on. They already have an opinion that we’re trying to change. This has at least three implications:
- We need to use a two-sided rather than a one-sided approach. That is, we need to concede that there are some valid arguments against individual preparedness – for example, the fact that the government has a substantial antiviral stockpile it didn’t used to have, is working toward an H1N1 vaccine, and is genuinely better prepared to cope (at least with a “mild” pandemic) than it was just a few years ago. Another key point that has to be conceded: If swine flu stays as mild as it has been so far (a big if), not all that much individual preparedness is likely to prove necessary. In our desire to see people prepare for the more severe pandemic that might (or might not) materialize, you and I are in the minority. It won’t work to ignore the majority’s best points.
- We also need to acknowledge and respectfully rebut the not-so-valid arguments against individual preparedness. The key here is “respectfully”; we’re playing donkey, and the core of that risk communication “game” is validating that people aren’t foolish to think what they think … before we tell them why we think they’re mistaken. Look again at your rebuttal of the view that individual stockpiling could lead to shortages or even to panic. You skip right to asserting how wrongheaded it is. Try conceding first that this view is widespread and natural, and that the burden of proof is on you to show why it’s erroneous.
- Perhaps most important, we need to be empathic about the emotional factors underlying many people’s reluctance to start preparing actively for a potentially severe pandemic.
- There have been warnings about impending doom before – including impending pandemic doom, and even (just a couple of weeks ago) impending swine flu doom. So far, no doom. Many people may feel a bit foolish, and more than a bit irritated, about having been gulled – and are understandably disinclined to "overreact" and feel foolish/gulled again.
- In the short term, nobody wants to look weird to the neighbors. (My wife and colleague Jody Lanard wears a mask in crowded places; I think it’s a sensible precaution – but I haven’t got the social courage to do likewise.)
- We all have enough things to worry about already….
Please notice that I have framed these empathic acknowledgments in terms of “many people” or myself; it’s not empathic to accuse others of feelings they may not want to acknowledge. (See my column on “Empathy in Risk Communication.”)
A final point: As more and more people have learned in recent weeks, the term “pandemic” refers to how widespread a contagious disease is, not how devastating it is. The odds are overwhelmingly in favor of the World Health Organization declaring Pandemic Phase 6 within days – quite possibly before this Guestbook response is posted. That will officially affirm that the H1N1 pandemic is underway. Many are worried that people will overreact to the Phase 6 declaration, for example by pressuring governments to close borders (a move that virtually all experts think would do more harm than good). In fact, there is pressure now on WHO to change its pandemic phase definitions for the second time in a month, in order to avoid having to declare a comparatively mild H1N1 pandemic a pandemic at all.
I have the opposite worry: that a pandemic will be declared and nothing much will change – and people will conclude that pandemics are no big deal. So they’ll be twice disillusioned. For years we “promised” a pandemic and none appeared. Finally, probably this week or next week, we will “deliver” a pandemic … and it will look for the moment like a non-event, a stunning anticlimax.
To avoid this additional disillusionment, I think we need to forewarn our loved ones – fast – that a Phase Six declaration won’t change things very much. The comparatively mild pandemic that seems to be emerging so far isn’t as insignificant as people have been led to imagine (see “Visualizing a mild pandemic”), but it’s not likely to require extensive personal stockpiles of food, water, medications, and other supplies. What makes you and me want to convince our family and friends (and governments and corporations) to do more pandemic prep isn’t the mild pandemic that will probably be declared very soon; it’s the more severe pandemic that could emerge from that mild pandemic sooner or later (or never). We would be well-advised to say so now.
Many pandemic preparedness websites have long discussions about the various approaches “preppers” have used to convince their loved ones to prepare for a potentially severe pandemic. For a distillation of pretty empathic responses to the most common skeptical questions, check out the “Frequently Asked Questions” link on the home page of getpandemicready.org. The site was developed with H5N1 bird flu in mind, but the principles and recommendations apply equally to H1N1 swine flu.
Audience segmentation for pandemic prep communications
I have been thinking about writing a column to describe the various audiences of pandemic preparedness communications (by which I mean preparing for a more severe pandemic – and I should start saying so every time), with messaging recommendations for each audience. I’ve been looking for survey data that might help me estimate the relative size of the audiences.
In the meantime, your comment leads me to take a first crack at the segmentation part of the job. What segments do the people we want to warn fall into? I’m going to use my inattentives/browsers/attentives/fanatics taxonomy as a starting point, but I’ll have to add some additional categories to make it work.
- Inattentives.
The inattentives are genuinely not paying attention to the emerging swine flu pandemic. At the extreme, they may actually be unaware of it altogether. More likely, they’re aware but uninterested. They’re following sports, or the arts, or politics … but not this.- Browsers.
The browsers are following swine flu in the media with some interest but no real involvement. They don’t feel it’s about them. You can’t say they have “decided” not to prepare; the possibility of preparing hasn’t really occurred to them yet.- Scoffers.
The scoffers believed from the outset that the reaction to swine flu was excessive. Even when the early news from Mexico looked like a severe pandemic might be imminent, they thought people were silly to worry. Now that the disease has turned out comparatively mild (so far), they feel vindicated.- Dupes.
The dupes took the early scary news from Mexico seriously. They may even have started preparing, or at least thought about it. So when the disease turned out comparatively mild (so far), they felt foolish and gulled – hoodwinked by fear-mongering officials and journalists. (For the record, I certainly don’t believe they were dupes. They do.)- Attentives.
Like the dupes, the attentives were very worried at first, and then became less worried when the news improved. Unlike the dupes, the attentives don’t feel foolish or gulled. They know the situation could turn alarming again at any moment. They’re being vigilant, and they’re preparing (or at least thinking about preparing, or already prepared).- Fanatics.
Like the dupes and the attentives, the fanatics were very worried at first. Unlike the dupes and the attentives, the fanatics never quite absorbed the news that the disease was turning out comparatively mild (so far). They think officials are underplaying or even hiding the seriousness of the situation. They’re not panicking (though people say they are), but they are a bit overwrought. They are of course preparing (or already prepared).- Deniers.
The deniers may masquerade as inattentives, scoffers, or dupes; that is, they claim to be unconcerned about the possibility of a severe pandemic. But what looks like apathy is actually its opposite. They can’t bear the thought of what might happen, or the feelings it arouses. So they have tripped a psychological circuit breaker and convinced themselves it can’t happen.
If you’re trying to sell pandemic preparedness, the attentives are your allies. The scoffers are your opponents.
The browsers and the dupes are your key target audiences, and they require quite different messaging. (In the first part of this answer, I made the assumption that your resistant family and friends are likelier to be dupes than browsers.)
What about the other three groups? The inattentives are pretty much a lost cause until things get worse, when they will belatedly move into another group. And the fanatics and the deniers are special cases, psychologically much more complicated than the other five groups. I suspect they are probably the two smallest groups.
Focus on the browsers and the dupes.